Translation and validation of cognitive failure questionnaire in Urdu among elderly
DOI:
https://doi.org/10.52567/trehabj.v10i01.143Keywords:
cognitive failure, cross cultural adaptation, psychometrics, UrduAbstract
Background: The Cognitive Failure Questionnaire (CFQ) is widely used self-reported instrument for assessing everyday cognitive lapses but no validated Urdu version is available.
Objective: to translate, culturally adapt the CFQ into Urdu (CFQ-U), and to evaluate the psychometric properties in the Urdu- speaking elderly population.
Methodology: The CFQ was translated and cross culturally modified into Urdu following the Consensus based standards for the selection of health measurement instruments using COSMIN criteria this included forward and backward translation, expert review, content validity assessment (CVI), and pilot testing to ensure semantic, conceptual, and cultural equivalence before finalizing the Urdu version (CFQ-Urdu). Total n=250 community dwelling participants with age ≥60 years completed the questionnaire. Test-retest reliability was assessed in n=70 participants, and they completed questionnaire twice after a week interval. In subsample of n=35 participants, construct validity was assessed. The Urdu CFQ measures subjective cognitive failures in daily life, not objective cognitive impairment. Therefore, in subsample of n=35 participants for construct validity, we used the Urdu versions of Beck Depression Inventory, Beck Anxiety Inventory, and Patient Health Questionnaire-9, as subjective cognitive complaints are theoretically and empirically associated with depression and anxiety. In contrast, Montreal Cognitive Assessment is a performance-based screening tool for objective cognitive impairment, which assesses a different construct than the CFQ. Internal consistency, content validity, construct validity, and exploratory factor analysis were evaluated by using the method of KMO, Barlett's test.
Results: The CFQ-U showed good internal consistency (Cronbach's α=0.74) and test-retest reliability (intra-class correlation coefficient=0.996). Three factor structure supported by exploratory factor analysis explained 48.6% of total variance. Non-significant and weak correlation was observed in between CFQ-U scores and anxiety, depression and general health measurement supporting discriminant validity. Small floor effect was identified with no ceiling effect.
Conclusions: The CFQ-U is a reliable and psychometrically valid instrument for assessing cognitive failures among elderly Urdu-speaking individuals. It can be useful for research applications and clinical screening in geriatric population.
INTRODUCTION
Cognitive failures, such as forgetfulness, lapses in attention, and action errors are subjective everyday cognitive lapses that are common among the elderly and may affect daily functioning, safety, and quality of life but they are distinct from MCI and dementia, which involve objective, cognitive decline [1,2]. Identification and assessment of cognitive failures is crucial step to mitigate their consequences and implement timely interventions [3]. It can be caused by several factors, such as age, gender, stress, sleep deprivation and demands of the job [4,5,6,7]. Mild cognitive impairment is a type of cognitive decline that is often linked to aging [8].
Cognitive failures can lead to a range of negative outcomes, including reduced functional ability, increased risk of falls, forgetting to turn off appliances, gait disturbances and decrease in daily activities performance [9]. Cognitive functions can compromise motor planning, balance, and coordination [10]. All this leads to reduced confidence in movement, promoting a sedentary lifestyle [9,10]. It is also associated with heightened emotional distress, including anxiety, frustration, and depression, further exacerbating the risk of social withdrawal and diminished quality of life [11]. They may also contribute to caregiver burden and increased healthcare utilization due to preventable incidents.
The Cognitive Failure Questionnaire (CFQ) is a widely used self-reported tool for assessing the frequency of cognitive failures. It was deemed as a detailed and widely utilized subjective outcome measure in different populations [12]. It is evident that CFQ is a commonly used and recognized metric because it has been translated to different languages, for example, Hebrew [13], German [14], Dutch [15], Italian [16], Brazilian [17] , Turkish [18] or Hungarian [19] and it has shown good psychometric properties in all of these languages.
Present study addresses that despite the international utility of CFQ, absence of its Urdu version constraints the accessibility to large group of aging population in Pakistan. Due to language barrier among older adults, use of instrument in non-native language may lead to inaccurate reporting of cognitive function. Increased prevalence of age-related cognitive decline in Pakistan along with limited mental health resources emphasizes the urgent need for validated and accessible tools. Validated Urdu version of CFQ which is culturally adapted is essential for accurate cognitive assessment among Urdu speaking elderly population. By translation and cross-cultural adaptation of CFQ into Urdu, and evaluation of its psychometric properties in representative sample of Urdu speaking elderly population in Pakistan will enable clinicians, researchers and policy makers for cognitive screening with a valid and reliable tool. In geriatric care region critical practical and methodological gap is also filled. The purpose of this study was to translate and culturally adapt the CFQ into Urdu (CFQ-U) using recognized methodologies, as well as to examine the translated version's psychometric properties in Urdu-speaking elderly population.
METHODOLOGY
Study DesignThis was a cross-sectional study aimed at the translation and psychometric and validation of Cognitive Failure Questionnaire into Urdu. The process was initiated after receiving consent from the developer of the original CFQ. The study was conducted from March 2023 to January 2024 in accordance with the Consensus-based Standards for the selection of health status Measurement Instruments (COSMIN) criteria [20]. Six steps and Sequential approach in the entire procedure was used for translation process [21]. Ethical approval for this study was obtained from the Research Ethics Committee (REC), Riphah College of Rehabilitation and Allied Health Sciences, Riphah International University, Islamabad under reference number Riphah-RCR&AHS-ISB/REC/MS-PT/01645. All procedures were conducted in accordance with the ethical standards of the institutional research committee and the Declaration of Helsinki. Written informed consent was obtained from all participants prior to their inclusion in the study.
ParticipantsTotal of n=250 community dwelling older adults by nonprobability purposive sampling technique, both male and female patients with age 60 years above fluent in understanding and reading Urdu, mentally alert to give consent and complete forms were recruited from community gathering areas like public parks, mosques, community centres in urban and peri-urban areas of Islamabad and Rawalpindi, Pakistan. Participants not capable to complete the questionnaire without any help or diagnosed with dementia or having any neurological/psychiatric impairment were excluded from the study. To calculate sample size for general psychometric testing and factor analysis, 10:1 subject to item ratio was calculate [25], so (25-items x 10) n=250 participants were recruited for this study which improves generalizability and external validity of findings to broader Urdu- speaking elderly population.
InstrumentsCognitive Failure Questionnaire: The cognitive failure questionnaire (CFQ), a self-report questionnaire was designed to assess everyday motor lapses, perception, and memory. The 25 items on the CFQ are divided into three categories: distractibility (items 8, 9, 10, 11, 14, 19, 21, and 25), forgetfulness (items 1, 2, 5, 7, 17, 20, 22, and 23), and false triggering (items 2, 3, 5, 6, 12, 18, 23, and 24). The responses from the patients are evaluated using a 5-point Likert scale, where higher scores indicate more cognitive dysfunction [12].
Beck Depression Inventory: The BDI has been used to assess the participants' depression symptoms. This scale comprises 21 items ranging from 0 to 3 to assess the cognitive, emotional, and vegetative symptoms of depression. Score ranges from 0 to 63, with higher scores indicating higher levels of depression symptoms and vice versa [22].
Beck Anxiety Inventory: This scale uses 21 items ranging from 0 to 3 to assess anxiety symptoms. Scores vary from 0 to 63, higher scores indicating higher levels of anxiety symptoms [23].
Patient Health Questionnaire: PHQ-9 assessing the frequency of nine depressed symptoms during the last two weeks, on a 4-point Likert scale, respondents must indicate how frequently each symptom occurs (0 being hardly at all to 3 being almost every day). In addition, if at least one symptom appears, they must also assess the extent to which it interfered with their ability to function at work, take care of their family, or interact with others. Elevated scores signify an increased degree of depression symptoms [24].
Step 1 - Forward Translation: Two fluent English speakers having Urdu as mother tongue and holds master's degree in Urdu independently translated the CFQ from English into Urdu.
Step 2 - Synthesis I: The translators and one researcher produced a consensus version by integrating the results of the two translated versions and addressing discrepancies.
Step 3 - Blind backward translation: The agreed-upon Urdu version was translated back into English by a professional translator holding master's degree in English who was blind to the original questionnaire and its concept.
Step 4 - Synthesis II: A multidisciplinary panel of experts including researchers, translators, and a professor of physiotherapy, examined every translation, and after consensus, agreed on idiomatic, semantic, experiential, and conceptual equivalency to obtain a pre-final CFQ.
Step 5 - Content validity: Content validity was assessed by experts on n=20 older adults for relevancy, simplicity, ambiguity and clarity of each item from 0 to 4 content validity index (CVI).
Step 6 - Pilot Testing/Cognitive Debriefing: n=30 subjects evaluated to ensure face validity in Urdu. The expert committee including researchers, translators, and a professor of physiotherapy, assessed all the feedback from this stage of the adaptation process, and consensus was made to develop the final version of CFQ in Urdu (CFQ-Urdu).
After informed consent was obtained, structured demographic questionnaire and translated version of CFQ were completed by participants. Using a computerized random number generator, randomly n=70 participants were selected and asked to complete after one-week CFQ-U again to evaluate test-retest reliability. Subset consisting of n=35 participants completed CFQ-U, beck anxiety inventory (BAI), beck depression inventory (BDI) and patient health questionnaire-9 (PHQ-9) for construct validity. All questionnaires were self-administered with research assistant availability to clarify instructions, in a controlled environment. This study was approved by the ethics review committee of Riphah International University, Islamabad. This study adhered to institute research guidelines and declaration of Helsinki.
BiasTo minimize selection bias, uniform inclusion and exclusion criteria were applied consistently to all participants. To address self-report bias, standardized and previously validated instruments were used, and participants completed questionnaires independently in a quiet setting. To reduce recall bias, participants were instructed to respond based on recent everyday cognitive experiences rather than distant memories. Potential cultural interpretation bias was addressed through a structured translation and cross-cultural adaptation process following established guidelines, including expert review and pilot testing. Data collection was administered by trained researchers. Despite these measures, the potential influence of self-report and cultural interpretation of cognitive complaints could not be eliminated and is acknowledged in the Limitations section.
Data AnalysisData analysis was performed using the Statistical Package and Service Solution (SPSS) version 23 with significance level (α) set at 0.05. Age and questionnaire scores were summarized by means and standard deviations. No categorization was applied for CFQ-U items and taken as ordinal. For exploratory factor analysis items were analysed as continuous. BAI, BDI, and PHQ-9 scores were taken as continuous to develop construct validity. Exploratory model test was used to assess confirmatory factor analysis.
Reliability: Based on expected ICC of 0.81, 95% CI and 80% minimum power, sample size for test re-test n=70 was calculated [26]. Intra class correlation coefficient was used for test- retest reliability. It was computed by using two- way mixed effects model with absolute agreement. ICC ≥0.80 is considered excellent reliability [27]. Cronbach's alpha was used to evaluate Internal consistency with ≥0.70 is considered acceptable [28].
Content validity: It is the extent to which an instrument's content accurately reflects the construct being assessed [29]. Content validity index was calculated by five clinical experts who rated each item on relevance, simplicity and clarity on 4-point scale, considering ≥0.78 acceptable. Floor and ceiling effects sizes were used to evaluate the content validity. If more than fifteen percent of the respondents obtained the lowest or highest potential total score, floor and ceiling effects are deemed to be present.
Factor analysis: Confirmatory factor analysis was conducted as secondary exploratory procedure to assess factor structure plausibility identified by exploratory analysis not for definitive confirmation of factorial validity. The suitability and importance of the data were assessed using Bartlett's test of sphericity (p<0.05) and Kaiser-Meyer-Olkin's measure of sample adequacy (KMO) ≥0.6. The total variance shown in our data was also determined via factor analysis, and since varimax rotation maintains the factors' uncorrelated nature, it was used in addition to the orthogonal rotation approach. Maintaining the eigenvalues >1 was deemed sufficient with item loadings ≥ 0.3 [29], the sample size adequacy was n=250.
Construct validity: Two variants of concept validity exist, the degree to which your measures agree with measures of related constructs is known as convergent validity. As opposed to the degree to which your measure is unconnected to or adversely correlated with measures of different constructs is known as discriminant validity [30]. To evaluate construct validity, participants completed four questionnaires: the translated CFQ-U, the BAI, the BDI, and the PHQ-9 in Urdu. For this measure, the Pearson coefficient correlation was computed by comparing the outcomes of the scales that were taken simultaneously. Thus, the values acquired aided in the questionnaire's validation. Excellent correlation values range from 0.81 to 1.0, very good correlation values from 0.61-0.80, good correlation values from 0.41-0.60, acceptable correlation values from 0.21-0.40, and poor correlation values from any value equal to or less than 0.20 [31]. The required sample size was n=35 to compute this.
RESULTS
Translation and Cross-Cultural Adaptation
During synthesis II determination, item 16 was modified for semantic clarity while preserving original conceptual meaning. No additional items were modified following pilot testing. All items were comprehendible, and clear in pre-final Urdu version as reported by participants.
Participant Characteristics
The study included n=250 participants. No participant was excluded, and no missing data was reported. The mean age of the participants was 64.3±4.56 years. Of the total sample, n=92(36.8%) was male and n=158(63.2%) were female. The mean score on the Urdu version of the Cognitive Failure Questionnaire (CFQ-U) was 40.4±14.04, suggesting a moderate level of self-reported cognitive failure.
Psychometric Properties
Reliability: The Cronbach alpha (α) of the CFQ-U was 0.74 exceeding the acceptable threshold, indicating the good internal consistency.
Test-retest reliability: The Intraclass Correlation Coefficients (ICC) for individual items range from 0.898 to 0.990, indicating high reliability across all items. A total score ICC was 0.996, reflecting excellent temporal stability. Reliability estimates have been reported as unadjusted values as no confounder adjustment was done. (Figure 1)
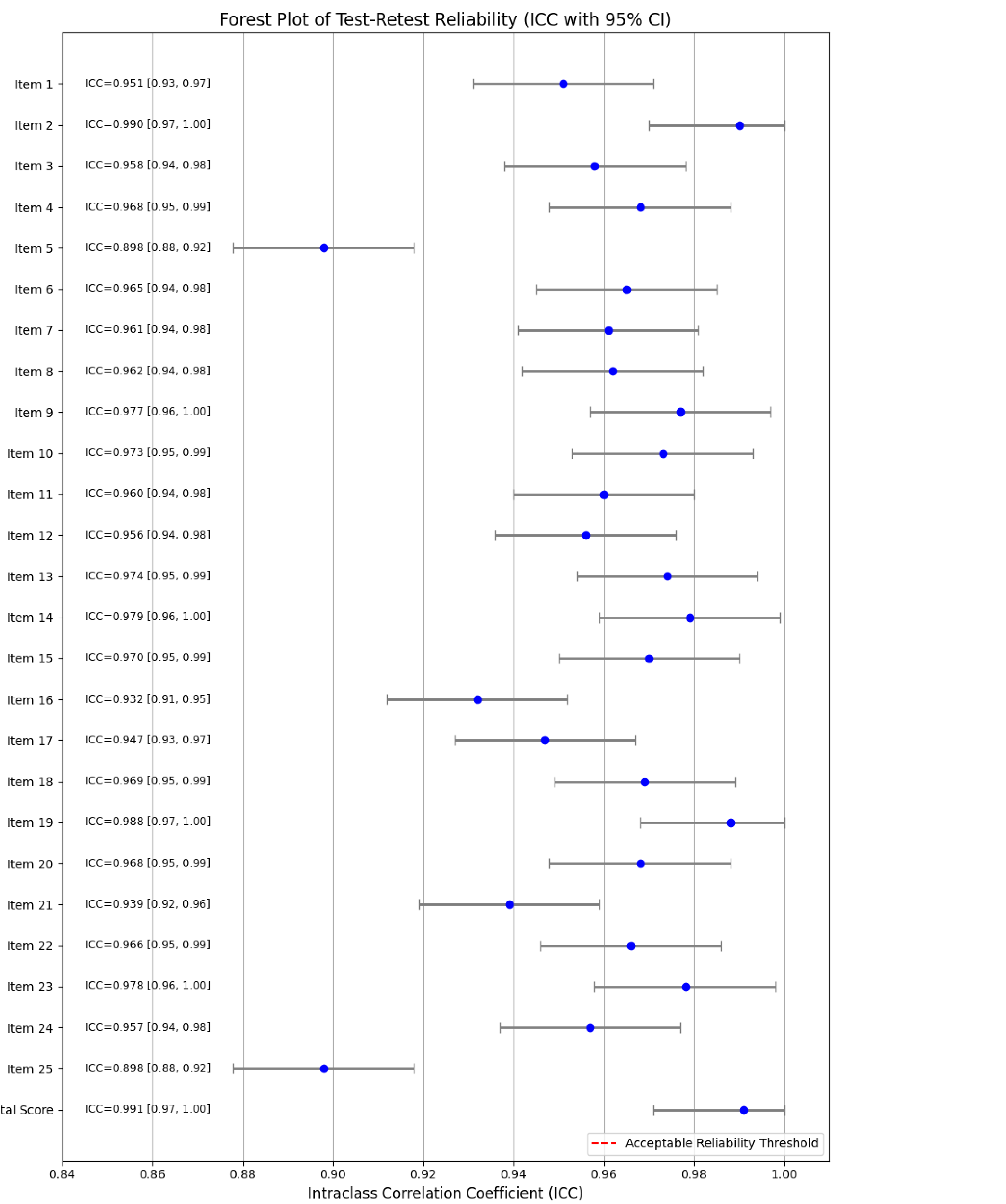 Figure 1: Forest Plot for CFQ-U ICC (95% CI)
Figure 1: Forest Plot for CFQ-U ICC (95% CI)
Content validity: it was assessed by experts' ratings for items relevance, clarity and simplicity. After analysis no ceiling effects on the total score of CFQ-U was observed. However, 16% of participants experienced floor effects suggesting very low frequencies of cognitive failure by small proportion of respondents.
Construct validity: The construct validity was assessed for subsample of n=35 participants by examining its Pearson correlations with the Beck Anxiety Inventory (BAI), Beck Depression Inventory (BDI), and Patient Health Questionnaire-9 (PHQ-9). The results showed a non-significant weak negative correlation between CFQ-U and BAI (r=-0.192, p=0.268), between CFQ-U and BDI (r=-0.014, p=0.936), and a very weak positive correlation between CFQ-U and PHQ-9 (r=0.011, p=0.949), supporting the discriminant validity of the CFQ-U by demonstrating that it measures a construct like forgetfulness and attention errors, distinct from anxiety and depression. (Figure 2)

Figure 2: Correlation heatmap (CFQ-U, BAI, BDI and PHQ)
Exploratory Factor Analysis
Exploratory factor analysis was conducted on a 25-item questionnaire measuring cognitive lapses in daily activities, using Principal Component Analysis with Varimax rotation. The KMO measure confirmed sampling adequacy (KMO=0.807), and Bartlett's test of sphericity showed significant correlations among variables (χ²(300)=2904.91, p<0.001).
Three factors emerged with eigenvalues >1, explaining 48.6% of the total variance. These factors were identified as (i) Everyday Cognitive Lapses, (ii) Spatial and Environmental Disorientation, and (iii) Communication and Interaction Errors. The model demonstrated simple structure with clear factor loadings, supporting the multidimensional nature of everyday cognitive failures. (table 1)
Table 1: Factor loading and Communality summery

The scree plot demonstrated a distinct inflection point after the third component, further supporting a three-factor solution. While most items loaded clearly on one factor, supporting a simple and interpretable structure, several items presented concerns. Specifically, Item 24 (Leave important letters unanswered) exhibited a negative and weak loading (-0.385) and low communality (0.355), suggesting limited contribution to any factor. Similarly, Item 25 (Forget why moved from room to room) demonstrated a cross loading on Factor 3 (-0.493) and the lowest communality (0.158) in the dataset, indicating it may not meaningfully reflect the latent constructs. In addition, items such as Item 17 (Fail to notice signposts) and Item 16 (Lose temper and regret) also showed low communalities (<0.30) and should be interpreted cautiously. (figure 3)

Figure 3: Scree plot
Confirmatory Factor Analysis (CFA)A Confirmatory Factor Analysis (CFA) was conducted as an exploratory model testing procedure to examine the three-factor structure identified through exploratory factor analysis could be tentatively supported in the present sample. The proposed model comprised of three latent constructs: Cognitive Lapses (measured by Items 15a, 24a, 22a, 19a, 23a, 20a, and 25a), Spatial Disorientation (Items 14a, 13a, 12a, and 11a), and Communication Errors (Items 8a, 6a, 5a, 4a, 2a, and 17a). Covariances among the latent variables were freely estimated.
The CFA results indicated that most of the observed variables loaded significantly onto their intended latent constructs. Standardized factor loadings range from -1.150 to 1.000 for Cognitive Lapses, -0.617 to 1.000 for Spatial Disorientation, and -0.723 to 1.000 for Communication Errors. Some negative loadings were observed, which may reflect reverse-worded items or opposing conceptual relationships within the factors. (table 2)
Table 2: Standardized Factor Loadings for the CFA Model

Partial discriminant validity between Cognitive Lapses, Spatial Disorientation, and Communication Errors was suggested by the small and negative covariance between the latent categories. In particular, there was a negative correlation between Cognitive Lapses and Communication Errors (covariance=-0.25) and Spatial Disorientation (covariance=-0.25) and communication error (covariance = 0.23), but Communication Errors and Spatial Disorientation similarly showed a negative covariance (covariance=-0.311). With 116 degrees of freedom, the chi-square statistic for model fit was 95.08. The Root Mean Square Error of Approximation (RMSEA) was 0.000, indicating excellent fit. Excellent match was indicated by the Root Mean Square Error of Approximation (RMSEA) of 0.000. However, the Tucker-Lewis Index (TLI=7.85) and Comparative Fit Index (CFI=6.846) were beyond the acceptable range, indicating care when assessing model fit. For future model comparisons, the Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) were 72.09 and 168.49, respectively. Future study should modify and re-evaluate the model because the observed CFI and TLI values may have been impacted by sample size constraints or abnormalities in estimate. (table 3)

Table 3: Summary of model fit statistics (Chi-Square, RMSEA, CFI, TLI, AIC, and BIC)

Figure 4: Path diagram illustrating the relationships among the constructs
A path diagram illustrating the relationships among the constructs is presented in Figure 4. The present CFA does not provide definitive evidence for proposed factor structure but offers an initial framework for future model refinement.
DISCUSSIONThe goal of current study was to translate, validate, and culturally modify the Cognitive Failures Questionnaire (CFQ) for the older population who speak Urdu. The results show that the Urdu version (CFQ-U) has good psychometric qualities that are quite similar to previous validations in other languages therefore, supporting its applicability in this population.
The CFQ-U displayed excellent test-retest reliability with an Intraclass Correlation Coefficient (ICC) of 0.996. This significantly exceeds reliability values reported in other language adaptations, such as the Hungarian version [19] (ICC=0.900) by Volosin et al. (2023) and the Dutch version [15] (r=0.83) by Merckelbach et al. (1996). Evaluation of temporal stability of CFQ-U scores is confirmed by these findings. The use of a brief, one-week delay between test administrations, which reduces memory deterioration and outside influences on participant responses, may be one explanation for this higher stability [19]. in older populations where, cognitive fluctuation is an issue, the high reliability across questions supports a steady evaluation of cognitive lapses across time.
With a preponderance of female participants, a Cronbach's alpha of 0.74 was acceptable and comparable to earlier validations, the Turkish version (α=0.91)[18], Brazilian Portuguese (α=0.906)[17], and Hungarian (α=0.92)[19]. These consistent results in many cultural contexts support the CFQ's cross-cultural robustness, the instrument's stability across gender distributions, and the goal of evaluating the CFQ-U's internal consistency.
The subjective nature of the CFQ-U questionnaire may be the cause of the floor effect observed in 16% of individuals. This is especially important for older persons, as cognitive declines may be ignored because of diminished metacognitive awareness, denied because of stigma, or normalized with aging [32].
Appropriate discriminant validity was shown by the CFQ-U. The CFQ-U evaluates a different construct from anxiety (BAI: r=-0.192), depression (BDI: r=-0.014), and general health symptoms (PHQ-9: r=0.011), according to weak, non-significant correlations. This contrasts with the original and other translations, where moderate to strong associations with BDI and BAI were found [18] in Turkish version. The lack of association in this study may indicate that older Urdu speakers have a distinct cultural understanding of cognitive lapses as age-appropriate or non-pathological forgetfulness, a theory that merits more investigation.
Three factors Everyday Cognitive Lapses, Spatial and Environmental Disorientation, and Communication and Interaction Errors were found by exploratory factor analysis (EFA) to account for 48.6% of the variance. This outcome is in line with the multifaceted nature of cognitive failures as demonstrated by earlier Turkish literature: five components [18], in English [16]: seven components, in Dutch: nine component [15]. The CFQ-U's content validity is supported by the establishment of three coherent variables that represent contextually relevant categories of cognitive lapses among the elderly. Items 24 (Leave crucial letters unanswered) and 25 (Forget why moved from room to room) showed atypical loadings and low communalities, which raised questions about their construct validity, especially in an older adult group. Instead of identifying fundamental cognitive deficiencies like memory or attention problems, item 24 can identify deficiencies in executive functioning or motivation. Instead of real cognitive impairment, these behaviours in older persons may potentially be a sign of social disengagement, low task engagement, or adaptive prioritizing [33]. Similar to item 25, forgetting one's objective after entering a new area is a relatively common occurrence that increases with age due to natural losses in prospective memory and attention control [34]. However, this behaviour may contribute to the poor discriminative power required for meaningful psychometric differences because it is so prevalent among older people. Previous research has shown that certain CFQ items perform poorly in elderly people because of decreased variability or cultural/contextual mismatch [35,36,37]. Therefore, these items may not adequately measure meaningful cognitive variability in old age samples and should be reconsidered in future translations of the scale aimed at older adults.
As a secondary, exploratory model testing method, Confirmatory Factor Analysis (CFA) was carried out. Although the RMSEA indicated a decent model fit (0.000), the TLI (7.85) and CFI (6.85) were excessively high and outside of acceptable ranges, which may have been caused by scaling or computational problems rather than model misfit. Furthermore, since comparable anomalies have been addressed in another study, some negative factor loadings (such as -1.150 for Item 20a) imply that some items may need to be reworded or reverse scored in order to fit with latent structures [38]. Confirmatory approaches are recommended by COSMIN for validation research involving larger samples and more advanced models. The results of the current study's CFA should be viewed cautiously and as a hypothesis generator rather than confirmation; yet, the results do not compromise the psychometric integrity of the study; rather, they highlight the difficulty of modelling subjective cognitive impairment in older populations.
With the exception of Item 16, which needed modification because of cultural idiomatic contradiction, translation and cross-cultural adaption were accomplished with little semantic distortion. The items' high level of clarity and relevance was confirmed by participant response, which is consistent with Beaton et al.'s cross-cultural questionnaire adaptation procedur [20].
While the CFQ-U demonstrates strong psychometric performance, some limitations should be acknowledged. The study was conducted in a specific region of Pakistan, which may not represent Urdu speakers from other sociocultural or rural settings. The sample predominantly consisted of females, which limits generalizability to male elderly. Moreover, results of CFA demonstrated instability in model fit indices. Sample size may have been insufficient for complexity of CFA model so findings should be interpreted with caution and should not be considered definitive confirmation for factor validity. Convergent validity with other cognitive screening tools was not considered in the study. These limitations can introduce bias in factor structure interpretation and hence restricts the external validity. Further, Cognitive status was assessed by only clinical judgment rather than any standardized tool (e.g., MMSE or MoCA), which may lead to potential misclassification.
Despite limitations, Urdu version of CFQ demonstrated strong reliability, acceptable factor structure and strong discriminant validity to fulfil the primary objective. CFQ-U can be cautiously applied to Urdu speaking older adults though further studies with diverse regional populations should be conducted for external validity.
CONCLUSIONThe CFQ-U is a reliable and valid tool for assessing cognitive failures among elderly Urdu-speaking individuals. It retains the structural and conceptual integrity of the original instrument and demonstrates sound psychometric properties. Future studies should include broader populations based on gender and different region to represent Urdu speakers from other sociocultural or rural settings. The very high ICC should be interpreted cautiously as short retest intervals may affect the ICC. Further, use standardized cognitive screening tools (e.g., MMSE or MoCA), and refine selected items to strengthen factor structure and generalizability.
DECLARATIONS & STATEMENTSAuthors Contribution
AK, AA: substantial contributions to the conception and design of the study.
AK: acquisition of data for the study.
AA, SW, and SKa: interpretation of data for the study.
AK, AA, SW, and SKa: analysis of the data for the study.
AK, AA, SK, and SK: drafted the work.
AK, AA, SKa, SW, WAS, and SKu: revised it critically for important intellectual content.
AK, AA, SKa, SW, WAS, and SKu: final approval of the version to be published and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors contributed to the article and approved the submitted version.
Ethical Statement
The study was approved by the Research Ethics Committee of Riphah College of Rehabilitation and Allied Health Sciences, Riphah International University, Islamabad (Ref: Riphah-RCR&AHS-ISB/REC/MS-PT/01645).
AI Use Statement
The authors used generative AI tools (e.g., ChatGPT, DALL·E) for language editing and figure generation. All content and interpretations were reviewed, verified, and approved by the authors.
Consent Statement
Written informed consent was obtained from all participants prior to data collection and for publication. The authors confirm that all participants voluntarily agreed to participate and that their confidentiality and privacy have been maintained throughout the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
None to declare.
Funding Sources
None to declare.
Conflicts of Interest
None to declare.
REFERENCES
- Carrigan N, Barkus E. A systematic review of cognitive failures in daily life: Healthy populations. Neurosci Biobehav Rev. 2016;63:29-42. [CrossRef] [PubMed]
- Tariot PN, Weingartner H. A psychobiologic analysis of cognitive failures. Structure and mechanisms. Arch Gen Psychiatry. 1986;43(12):1183-8. [CrossRef] [PubMed]
- Simpson SA, Wadsworth EJ, Moss SC, Smith AP. Minor injuries, cognitive failures and accidents at work: incidence and associated features. Occup Med (Lond). 2005;55(2):99-108. [CrossRef] [PubMed]
- Linden, D. V. D., Keijsers, G. P. J., Eling, P., & Schaijk, R. V. (2005). Work stress and attentional difficulties: An initial study on burnout and cognitive failures. Work & Stress, 19(1), 23–36. [CrossRef]
- Relationship between sociodemographic factors and cognitive failures among employees. (2023). Eur. J. Humanit. Soc. Sci. 3(1), 16-22. [CrossRef]
- Wadsworth EJ, Moss SC, Simpson SA, Smith AP. Psychotropic medication use and accidents, injuries and cognitive failures. Hum Psychopharmacol. 2005;20(6):391-400. [CrossRef] [PubMed]
- Wanleenuwat P, Iwanowski P, Kozubski W. Alzheimer's dementia: pathogenesis and impact of cardiovascular risk factors on cognitive decline. Postgrad Med. 2019;131(7):415-422. [CrossRef] [PubMed]
- Ward A, Arrighi HM, Michels S, Cedarbaum JM. Mild cognitive impairment: disparity of incidence and prevalence estimates. Alzheimers Dement. 2012;8(1):14-21. [CrossRef] [PubMed]
- Zhang T, Yang C, Shu G, Gao C, Ma H, Zou L, Zuo J, Liu S, Yan J, Hu Y. The direct and mediating effects of cognitive impairment on the occurrence of falls: a cohort study based on community-dwelling old adults. Front. Med. 2023 8;10:1190831. [CrossRef] [PubMed]
- Montero‐Odasso M, Speechley M. Falls in cognitively impaired older adults: implications for risk assessment and prevention. J. Am. Geriatr. Soc. 2018;66(2):367-75. [CrossRef]
- Lee JH, Luchetti M, Aschwanden D, Sesker AA, Strickhouser JE, Terracciano A, Sutin AR. Cognitive impairment and the trajectory of loneliness in older adulthood: evidence from the health and retirement study. J Aging Health. 2022;34(1):3-13. [CrossRef] [PubMed]
- Broadbent DE, Cooper PF, FitzGerald P, Parkes KR. The cognitive failures questionnaire (cfq) and its correlates. Br J Clin Psychol. 1982;21(1):1-16. [CrossRef] [PubMed]
- Meiran N, Israeli A, Levi H, Grafi R. Individual differences in self reported cognitive failures: The attention hypothesis revisited. Pers Individ Dif. 1994 1;17(6):727-39. [CrossRef]
- Klumb PL. Cognitive failures and performance differences: validation studies of a German version of the cognitive failures questionnaire. Ergonomics. 1995;38(7):1456-67. [CrossRef] [PubMed]
- Merckelbach H, Muris P, Nijman H, de Jong PJ. Self-reported cognitive failures and neurotic symptomatology. Pers Individ Dif. 1996 Jun 1;20(6):715-24. [CrossRef]
- Di Nocera F, Ferlazzo F, D’Olimpio F. Is ‘error proneness’ specific to errors? Predictive validity of the cognitive failures questionnaire. Int. J. Hum. Factors Ergon. 2014 1;3(2):208-25. [CrossRef]
- de Paula JJ, Costa DS, Miranda DM, Romano-Silva MA. Brazilian version of the cognitive failures questionnaire (cfq): cross-cultural adaptation and evidence of validity and reliability. Braz J Psychiatry. 2018;40(3):312-315. [CrossRef] [PubMed]
- Eser HY, Inan MY, Kucuker MU, Kilciksiz CM, Yilmaz S, Dincer N, Kilic O, Ercan AC, Aydemir O. Development, validity and reliability of the 4-point Likert Turkish version of cognitive failures questionnaire.
- Volosin M, Hallgató E, Csábi E. Validation of the Hungarian version of the cognitive failures questionnaire (CFQ). Heliyon. 2023;10(1):e12910. [CrossRef] [PubMed]
- Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine (Phila 1976). 2000 15;25(24):3186-91. [CrossRef] [PubMed]
- elamin s. Investigating the use of online bilingual resources by translation students: the vertical/sequential model revisited. J. Transl. Lit. Stud. 2023;17(7):4.
- Jackson-Koku G. Beck Depression Inventory. Occup Med (Lond). 2016;66(2):174-5. [CrossRef] [PubMed]
- Oh H, Park K, Yoon S, Kim Y, Lee SH, Choi YY, Choi KH. Clinical Utility of Beck Anxiety Inventory in Clinical and Nonclinical Korean Samples. Front Psychiatry. 2018;4;9:666. [CrossRef] [PubMed]
- Manea L, Gilbody S, McMillan D. A diagnostic meta-analysis of the Patient Health Questionnaire-9 (PHQ-9) algorithm scoring method as a screen for depression. Gen Hosp Psychiatry. 2015;37(1):67-75. [CrossRef] [PubMed]
- Anthoine E, Moret L, Regnault A, Sébille V, Hardouin JB. Sample size used to validate a scale: a review of publications on newly-developed patient reported outcomes measures. Health Qual Life Outcomes. 2014;9;12:176. [CrossRef] [PubMed]
- GUTTMAN L. A basis for analyzing test-retest reliability. Psychometrika. 1945;10:255-82. [CrossRef] [PubMed]
- Balk EM, Gazula A, Markozannes G, Kimmel HJ, Saldanha IJ, Resnik LJ, Trikalinos TA. Lower limb prostheses: measurement instruments, comparison of component effects by subgroups, and long-term outcomes [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018. [PubMed]
- Henson RK. Understanding internal consistency reliability estimates: A conceptual primer on coefficient alpha. Meas. Eval. Couns. Dev. 2001;34(3):177-89. [CrossRef]
- Swisher LL, Beckstead JW, Bebeau MJ. Factor analysis as a tool for survey analysis using a professional role orientation inventory as an example. Phys Ther. 2004;84(9):784-99. [PubMed]
- Colliver JA, Conlee MJ, Verhulst SJ. From test validity to construct validity … and back? Med Educ. 2012;46(4):366-71. [CrossRef] [PubMed]
- Schijven M, Jakimowicz J. Construct validity: experts and novices performing on the Xitact LS500 laparoscopy simulator. Surg Endosc. 2003;17(5):803-10. [CrossRef] [PubMed]
- Tsouvala A, Katsouri IG, Moraitou D, Papantoniou G, Sofologi M, Nikova A, Vlotinou P, Tsiakiri A, Tsolaki M. Metacognitive awareness of older adult drivers with mild cognitive impairment: relationships with demographics, subjective evaluation of cognition, and driving self-efficacy. Behav Sci (Basel). 2024;6(6):483. [CrossRef] [PubMed]
- Knight MJ, Baune BT. Executive function and spatial cognition mediate psychosocial dysfunction in major depressive disorder. Front Psychiatry. 2018;29;9:539. [CrossRef] [PubMed]
- Craik FIM, Henry JD. Age-related changes in everyday prospective memory. In: Logie R, et al., editors. Memory in Science for Society: There is nothing as practical as a good theory. Oxford: Oxford University Press; 2023. [CrossRef]
- Nielsen TR. Cognitive assessment in culturally, linguistically, and educationally diverse older populations in Europe. Am J Alzheimers Dis Other Demen. 2022;37. [CrossRef] [PubMed]
- Schneider S, Lee PJ, Hernandez R, Junghaenel DU, Stone AA, Meijer E, Jin H, Kapteyn A, Orriens B, Zelinski EM. Cognitive functioning and the quality of survey responses: an individual participant data meta-analysis of 10 epidemiological studies of aging. J Gerontol B Psychol Sci Soc Sci. 2024;79(5):gbae030. [CrossRef] [PubMed]
- Czerwinski-Alley NC, Chithiramohan T, Subramaniam H, Beishon L, Mukaetova-Ladinska EB. The effect of translation and cultural adaptations on diagnostic accuracy and test performance in dementia cognitive screening tools: a systematic review. J Alzheimers Dis Rep. 2024;8(1):659-675. [CrossRef] [PubMed]
- Rast P, Zimprich D, Van Boxtel M, Jolles J. Factor structure and measurement invariance of the cognitive failures questionnaire across the adult life span. Assessment. 2009;16(2):145-58. [CrossRef] [PubMed]

Submitted
Accepted
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 Aniqa Khalid

This work is licensed under a Creative Commons Attribution 4.0 International License.
Authors retain copyright and grant the journal right of first publication and allows others to share the work with an acknowledgment of the work’s authorship and initial publication in this journal. No use, distribution or reproduction is permitted which does not comply with these terms.