Effects of low impact elliptical training on knee osteoarthritis outcomes and knee joint space
DOI:
https://doi.org/10.52567/trehabj.v8i04.84Abstract
Background: Different physical therapy treatment strategies are used to decrease the symptoms and reduce the severity of knee Osteoarthritis (OA). Low-impact elliptical training is like mobilizations, which increase nourishment and contribute to increased joint space. Objective: To determine the effects of low-impact elliptical training on knee osteoarthritis (OA) outcomes and knee joint space.
Methods: Data for the randomized controlled trial (NCT05977374) was collected from 28 participants through a non-probability convenience sampling technique and randomized into group A: which received low-impact elliptical training along with conventional therapy, and group B: which received traditional physical therapy for 12 weeks. The outcomes were checked through a knee injury and Osteoarthritis Outcome Score (KOOS) pre and post-treatment at the 6th and 12th week and knee space was measured by X-rays pre and post-treatment at the 12th week only.
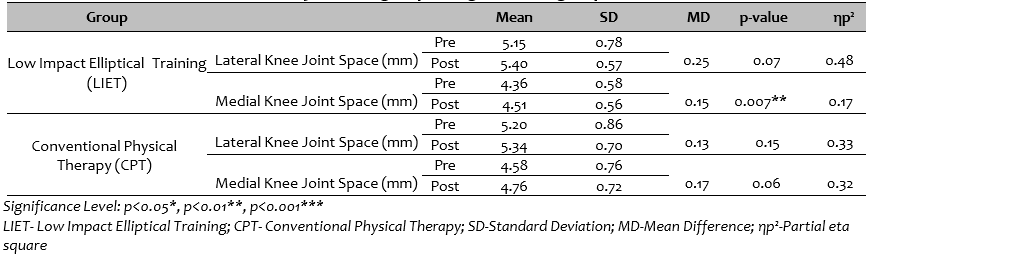
Results: 51.92±9.106 years was the mean age of group A study participants, and 50.29±5.483 years for group B. Within-group analysis, all domains of the KOOS for the low-impact elliptical training group showed significant improvement (p≤0.005). Between-group analyses, all the domains of the KOOS showed a non-significant difference with p≥0.05. In the between-group analysis of the knee joint width of the medial and lateral spaces in pre- and post-observation, there was no significant difference noted, but within the group, significant improvement (p=0.007) was observed in the medial space for the LIET group only
Conclusions: Elliptical training can be used to intervene in individuals with grade 1 and 2 knee osteoarthritis compared to conventional physical therapy for the alleviation of pain, stiffness, ADLs, sports, and QOL. Moreover, it may improve knee joint space.
INTRODUCTION
Knee osteoarthritis (OA) is a chronic degenerative disease affecting millions of people worldwide, particularly those above 60 years of age[1, 2]. Different factors, including trauma or joint injury, repetitive actions like squatting and kneeling, mechanical stressors, obesity, old age, sex, lifestyle, calcium deficiency, metabolic diseases like diabetes, and genetic factors, can contribute to knee OA[3]. Knee osteoarthritis can result from the degradation of cartilage, the formation of osteophytes, and the reconstruction of the subchondral bone[4]. Generally, knee OA is diagnosed by physical examination, X-ray images, MRI scans, and arthroscopy[5].
To decrease the symptoms and severity level of knee osteoarthritis, physical therapy is one of the treatment strategies that can be employed [6]. Grade 1 and 2 mobilization can reduce pain and improve joint function by promoting blood flow, improving nutrient delivery, increasing joint lubrication, and reducing stress on the joint surfaces. Additionally, by increasing the range of motion and promoting joint flexibility, they may help decrease the compressive forces on the joint, hence helping to improve joint space. Low-impact exercises such as swimming, cycling, or elliptical machines can facilitate the maintenance of knee homeostasis. These exercises initiate a cycle of optimally promoting knee chondrocyte production and regenerating knee cartilage through the cyclic compression loading technique, which enhances blood flow, oxygen, and nutrient supply[7].
Elliptical training is a popular fitness tool due to its ease of use and low risk of injury, which simulates the motion of walking or running while reducing the impact on joints [8] [9]. It has been found to have positive effects on knee osteoarthritis by decreasing knee varus and improving physical function and walking ability in individuals after total hip arthroplasty [10]. Off-axis elliptical training also reduces pain, improves knee function, and enhances lower extremity neuromuscular control in older adults [11]. Modified elliptical trainers with a converging footpath and reduced inter-pedal distance have different impacts on knee joint kinematics depending on the direction and incline of the exercise. Elliptical training puts less strain on the joints than high-impact exercises and protects knees from stressful impact [12].
As elliptical training employs the same cyclic process of compressive loading as manual knee joint mobilizations, the mobilizations are mostly performed manually, and active participation of the patient is limited. Elliptical training, on the other hand, would allow the patient to engage actively and support cartilage recovery in knee osteoarthritis. Until now, limited information has been available on the effects of elliptical training on knee space changes in knee OA, so this study assessed the effects of elliptical training on knee joint space and knee OA outcomes.
MATERIAL AND METHODS
Study Design & Setting: It was a single-blinded, randomized clinical trial (NCT05977374) conducted at the Islamabad Physical Therapy and Rehabilitation Centre (IPRC-21-01-2022-23), Rawalpindi, Pakistan. The study was completed within 1 year from January 2022-Feburary 2023 and approval was taken from the research and ethical committee (REC) of the Faculty of Rehabilitation and Allied Health Sciences (RIPHAH/RCRS/REC/Letter-01238) Riphah International University.
Participants: Selected participants were between the ages of 40 and 65, both male and female, with knee osteoarthritis (OA) of grades 1 and 2. Participants were ineligible if they had any recent musculoskeletal ailments, such as trauma or fractures of the lower limb. Individuals suffering from low back discomfort, sciatica, acute infections, or fever were excluded. Participants who were using supplements or drugs that might potentially interact with the findings from the research were also eliminated. Finally, the existence of any knee joint abnormalities was a significant determinant of exclusion.
Sample Size: Using G-Power, keeping the effect size small (0.24), α error margin at 0.05 and to avoid β error probability, the power (1- β) was set at 0.95%, and the sample size calculated was n = 28. A total of n=100 patients were assessed for eligibility through the non-probability convenience sampling technique and 28 participants fulfilled the inclusion criteria.
Randomization: The envelop sealed method using a computerized random number generator was used for randomization. An individual who was not directly involved in the study did the random allocation. The random numbers were then written on the index cards and placed in a thick and opaque sealed envelope before the start of the study. After obtaining written informed consent, the physical therapist opened the envelope and provided the respective interventions to the patients. As the assessed patient was blinded to the intervention so the study was single-blinded.
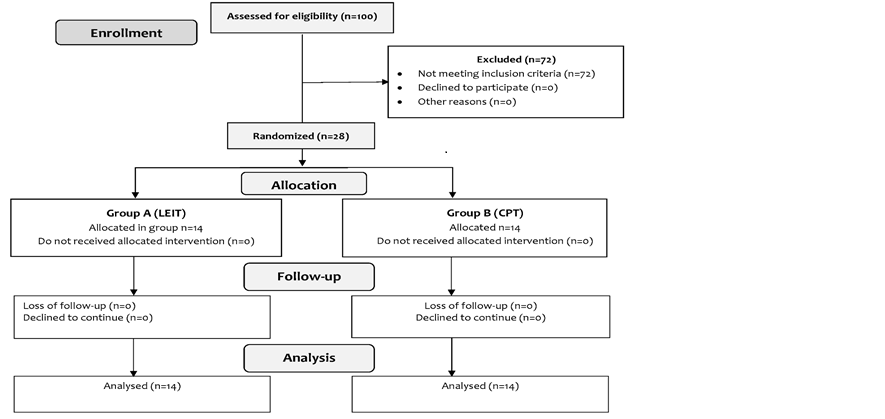
Figure 1: CONSORT diagram
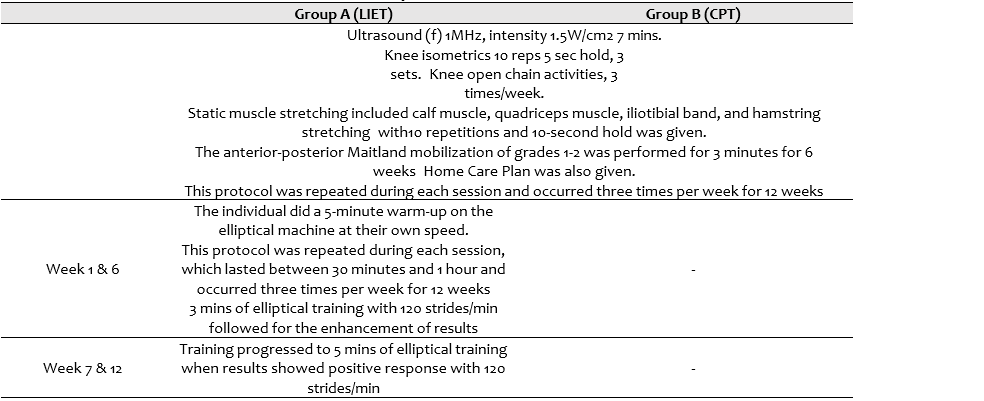
Intervention: 60-minute session was given to each patient 3 times per week and was given for 12 weeks. Data was collected at baseline, after 6 weeks, and then after 12 weeks for KOOS, but knee joint space was measured by X-ray at baseline and after 12 weeks.
Treatment Group A (Conventional Physical Therapy and low impact Elliptical Training): received electrotherapy sessions (Ultrasound (f) 1 MHz, intensity 1.5W/cm2, 7 mins), isometric exercises (10 reps, 5 sec hold, 3 sets), and open chain activities for 40–50 minutes, 3 times per week. Before and following elliptical training, each participant undertook static stretching exercises. Static muscle stretching included calf muscle, quadriceps muscle, iliotibial band, and hamstring stretching with10 repetitions and 10-second hold for each leg.
The individual did a 5-minute warm-up on the elliptical machine at their own speed. Once the individual was acquainted with the equipment, the 3-minute elliptical training began at a predetermined rate. This protocol was repeated during each session, which lasted between 30 minutes and 1 hour and occurred three times per week for 12 weeks. For weeks 1–6, 3 minutes of elliptical training with 120 strides per minute were followed for the enhancement of results. For weeks 7–12, training progressed to 5 minutes of elliptical training with 120 strides per minute.
Treatment Group B (Conventional Physical therapy): The conventional group received the electrotherapy (Ultrasound (f) 1MHz, intensity 1.5W/cm2, 7 mins) and isometric exercises (10 reps, 5 sec hold, 3 sets), knee open chain activities 3 times/week, and stretching exercises were performed. The anterior-posterior Maitland mobilization of grades 1-2 were performed for 3 minutes for 6 weeks, then after that, the oscillation time was increased to 5 minutes, and a home plan was given.
Table 1: Description of intervention
Assessments: The researchers considered the ethical, legal and regulatory norms and standards for this research according to the Declaration of Helsinki as a statement of ethical principles for medical research involving human subjects, including research on identifiable human material and data. For data collection, a demographic questionnaire with KOOS was used. Additionally, x-rays were used as a third method to check the existence of knee OA grades and post-treatment improvements in the knee joint space with radiant software. The five patient-relevant aspects of the KOOS were graded separately: pain (9 things); symptoms (7 items); ADL function (17 items); sport and recreation function (5 items); and quality of life (4 items). All items have five possible answers being rated from 0 to 4.The random effects intraclass correlation coefficients for pain, 0.93 for symptoms, 0.75 for activities of daily living, 0.81 for sport and recreation function, and 0.86 for knee-related quality of life were all considered high [13].
Radiant DICOM (Digital Imaging and Communications in Medicine) Viewer is a medical image processing and display application that uses the DICOM protocol [14]. DICOM software are used to examine a variety of imaging techniques, including digital radiography (CR, DX), magnetic resonance (MRI ), digital angiography (XA), computed tomography (CT), ), and ultrasound (US, IVUS) etc.[15] Radiant software is designed to analyze a wide range of digital data formats, including 2D and 3D images. The ability to view CR, CT & MRI studies on your PC using VR would allow medical practitioners to better evaluate a disorder along its 3D morphology and also help in determining a treatment plan[16]. We use Radiant DICOM for viewing digital X-rays of the knee joint and have found it, an excellent tool for analyzing knee osteoarthritis. The radiographs of the anterior-posterior and lateral views of the knee joint were taken [17]. Then these images were transferred to DVD and different dimensions of knee joint space width (KJSW) were measured from digital X-ray film with the help of computer image measuring software at baseline and after 12 weeks.
Statistical methods: Descriptive statistics were used to summarize the study findings and were subsequently presented in tables and graphs. A mixed ANOVA with partial eta squared (ηp2) as the effect size was used to examine the interaction between interventions and the level of assessment because non-parametric tests were appropriate for the data. A one-way ANOVA test was used to analyze changes over time for between-group comparisons. The RM-ANOVA test was used for within-group comparisons. The data was analyzed using SPSS (v-20) with p<0.05 as a significant level.
RESULTS
The mean age of study participants of Group A was 51.92±9.106 years, whereas Group B had 50.29±5.483 years. The gender (p=o.12) and the BMI (p=0.54) are normally distributed in both groups. (Figure 2 & 3)
While assuming the sphericity, there is no homogeneity in the variance, whether the sphericity was assumed or not, there is no significant difference in the individual in the domain of KOOS with the level of assessments. There is no significant interaction effect regarding KOOS, pain {F= 1.058(2, 52), p-value 0.346}, symptoms {F= 0.053 (2, 52), p-value 0.608}, ADLs {F= 1.379 (2, 52), p-value 0.261}, sports {F= 2.394 (2, 52), p-value 0.101} and QOL {F= 1.177 (2, 52), p-value 0.316}. (Figure 5)
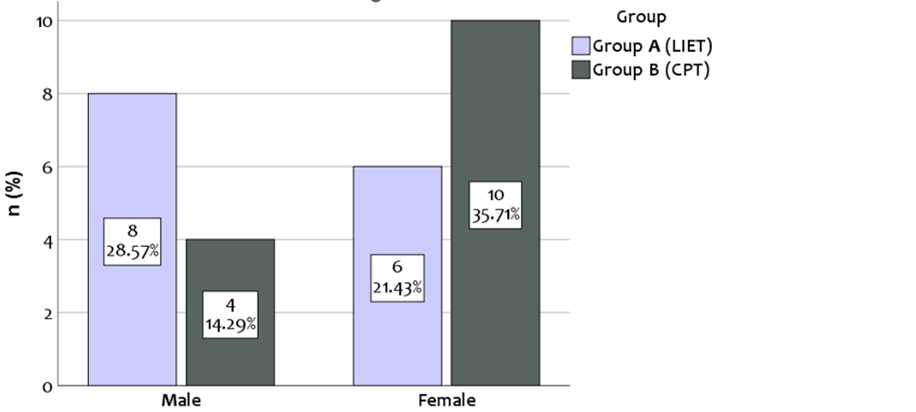
Figure 2: Gender Based distribution between Interventions
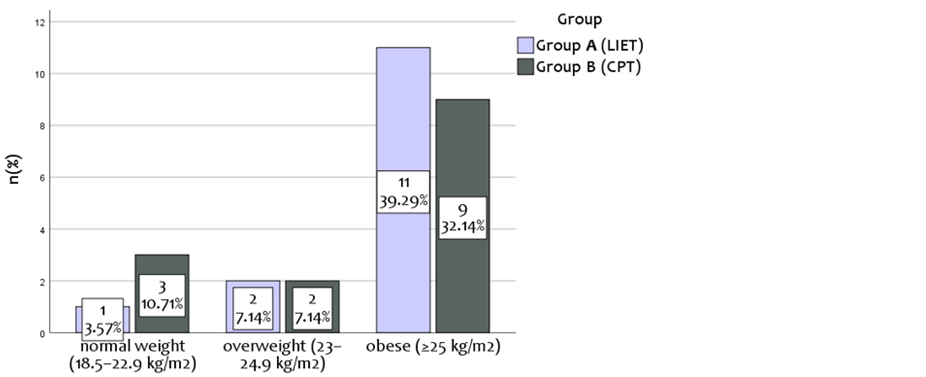
Figure 3: BMI distribution between interventions
Within-group analysis, the domains of the KOOS for Low Impact Elliptical training there is no significant difference within the groups in all its variables, pain, stiffness, ADLs, Sports, (p> 0.005) except QOL of Conventional Physical therapy training initially there was a no improvement from baseline to week 6 then from 6th week to 12th week, but generalized improvement has been seen from baseline to 12 week {F= 10.855(1.427, 18.55), p-value 0.002, ηp2=0.455}. However, an overall improvement has been observed within the group of CT. (Table 3).
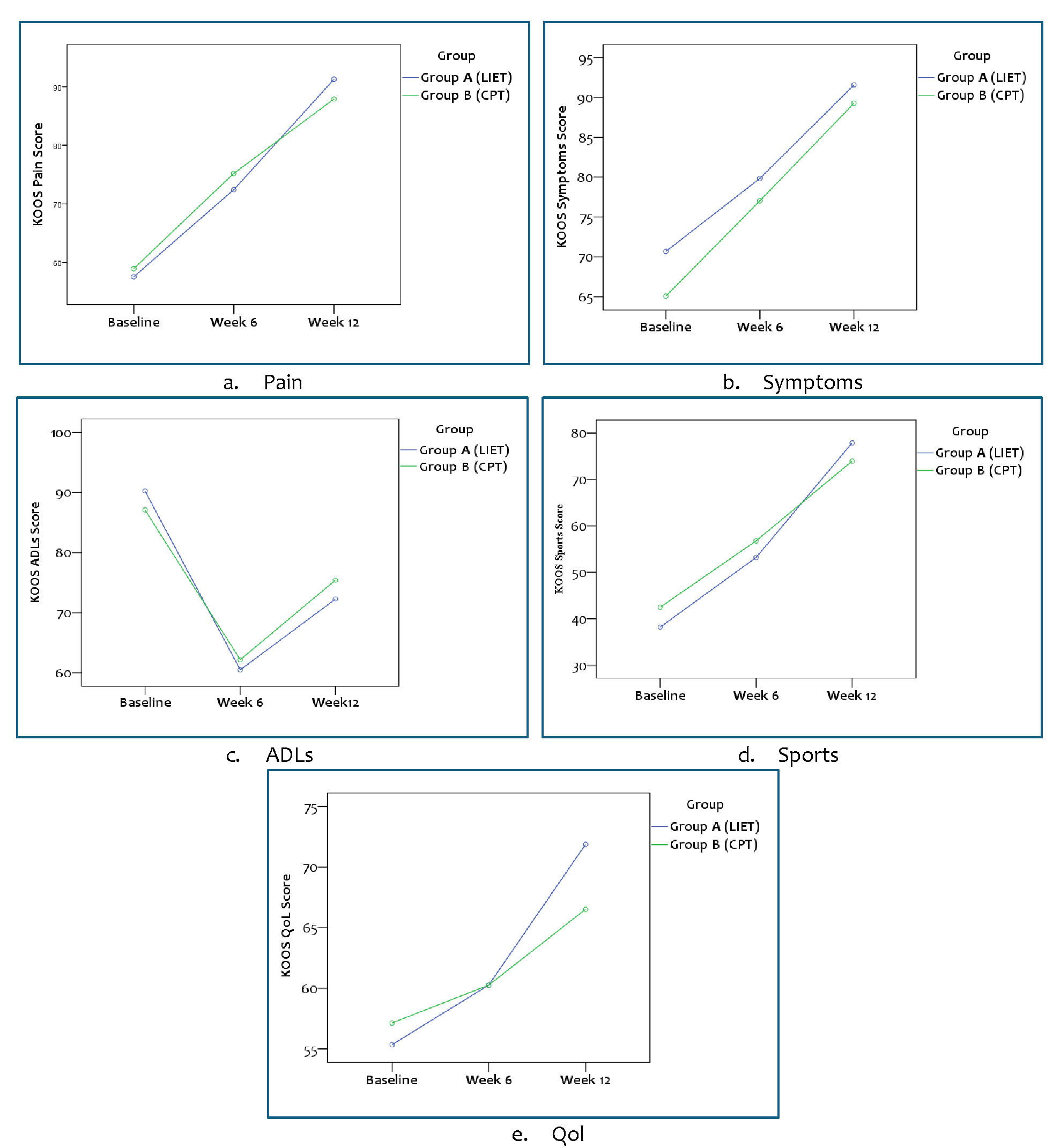
Figure 4: Interaction effects of intervention with level of assessment
Between-group analysis performed by one-way ANOVA which is explained in detail in Table 3, shows that in all the domains of the KOOS, there is no significant difference observed regarding pain, stiffness, ADLs, sports, and QOL with p≥0.05. From the baseline to the 6th week till the 12th week, better results have been documented from both groups. The between group analysis of the Knee joint width of the medial and lateral spaces in pre and post observation, in which there was no significant difference noted but with-in the group significant improvement was observed. Illustration showed in Table 4 & 5.
Table 2: With-in group (Main effects) changes in both groups
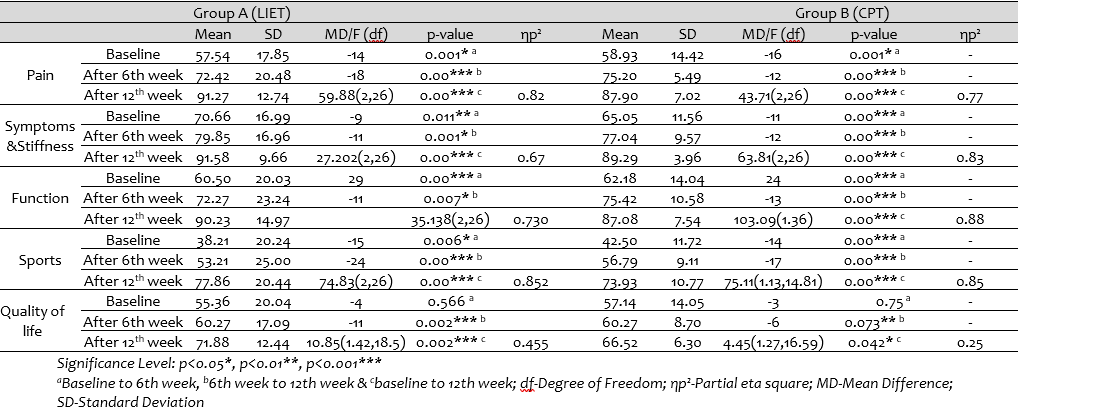
Table 3: One way ANOVA for between group analyses at three different points
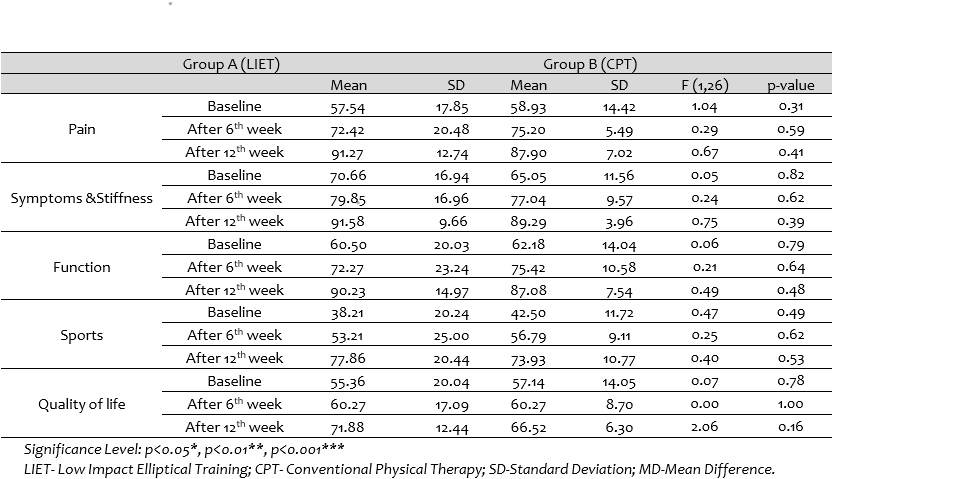
Table 4: Between the group changes in both groups.
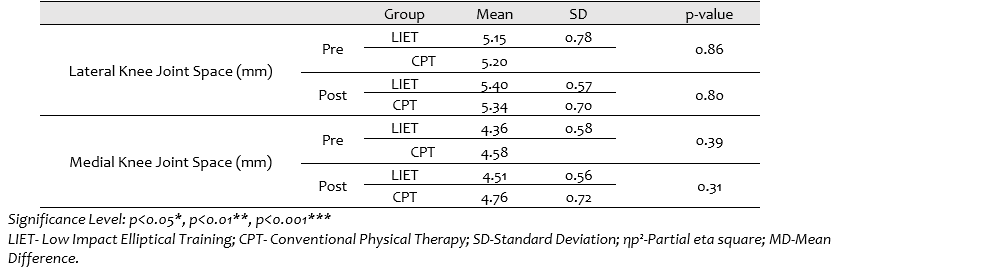
Table 5: With-in group changes in both groups.
DISCUSSION
The primary goal of the present study was to assess the effects of Low-impact elliptical training on knee joint space and the outcomes of Knee OA. According to the results of the present study, the mean age of participants was 51 years. Pain, stiffness, ADLs, sports, and QOL were significantly improved for the LIET group and the conventional treatment group, with no significant difference between the two groups, but the knee joint space showed significant improvement in the LIET group only. Hence, standard elliptical training generates peak knee valgus angle difference, impacting knee kinematics.
A study conducted on patella femoral pain patients using an off-axis elliptical training programmer showed a significant decrease in foot plate pivoting angle and sliding distance. It also showed improvement in lower limb off-axis control and single-leg hop distance by 0.2 meters.[18] With an elliptical machine, peak tibial forces are reduced as compared to running, which indicates a low loading rate and further enhancement on the medial side can be done by employing a larger step width on a regular elliptical machine[19]. In a recent study elliptical training showed the same positive outcomes in knee osteoarthritis. The possible reason behind that increased proprioception with minor weight-bearing slows the progression of cartilage abnormalities reduced pain, and improved knee function.
Different studies assessed the effects of different exercise interventions on knee cartilage health and related biomarkers. Bricca et al. evaluated the impact of exercise on articular cartilage health through systemic review in people with OA of the knee and found that loading interventions can lead to positive cartilage modifications and also have positive effects on glycosaminoglycan in knee cartilage [20]. Similar findings were also obtained in a recent trial in which knee outcomes and knee joint space were significantly improved in the elliptical training group. Knee ROM is also markedly improved in the elliptical training group. Cyclic compression puts less stress on the knee joint than high-impact exercises. During compression, fluid is taken from the synovial membrane, and during decompression, cartilage resorbs various nutrients and oxygen. This fluid then enters the extracellular matrix (ECM), where it circulates to chondrocytes at diverse tissue depths and facilitates cartilage development in OA patients[21, 22].
A 48-month cohort research indicated that people who used elliptical training generated more cartilage than those who did physical exercise [12]. Certain studies also showed promising outcomes and improved quality of life with minimal loading of joints by improving the health of knee joint cartilage[23]. In the present study, medial knee joint space in the elliptical group improved significantly. Recent studies also align with the results of previous studies showing peak knee valgus angle difference and reduction in knee osteoarthritis symptoms. Elliptical training involves a low-impact, weight-bearing exercise providing more space for the joint to move without excess compression or friction. Elliptical training has positive effects on joint biomechanics. It strengthens the muscles, such as the quadriceps and hamstrings, improving the blood circulation of the muscles around the knee joint to provide necessary oxygen and nutrients to the joint, enhancing tissue repair and reducing inflammation, which can contribute to increased joint space [24].
A systematic review reported positive effects of exercises on the outcomes of knee osteoarthritis patients[25]. A systematic review reported positive effects of resistance exercise on activities of daily living and knee outcomes [26]. In the present study, the conventional group, received electrotherapy, isometrics, open-chain exercises, and mobilizations and showed significant positive effects on knee outcomes. Exercise and Mobilization techniques can reduce pain and improve joint function by promoting blood flow and nutrient supply to cartilage. It helps in reducing inflammation and increasing flexibility of the knee joint [27].
Primorac et al. reviewed the pathogenesis of knee osteoarthritis and non-operative therapeutic considerations and found that exercise therapy results in significant improvements in KOOS and WOMAC, indicating the positive impact of exercise therapy Similarly, an RCT compared the effectiveness of manual therapy versus neuromuscular training by using VAS, WOMAC, and goniometry and concluded that manual therapy is more effective to decrease pain and physical disability as compared to neuromuscular treatment. A systematic review reported that manual therapy, when combined with exercises can be effective in reducing knee-specific impairments and improving overall QoL in knee osteoarthritis persons [28]. In a recent trial, grade I and II mobilizations were applied to the conventional group and resulted in positive effects on knee outcomes [29]. Grade 1 and 2 mobilization techniques may help to decrease the compressive forces on the joints and promote better alignment of the knee joint surface [30].
Romanowski et al. found that manual therapy(post-isometric relaxation and joint mobilization) interventions led to clinical benefits for knee pain reduction and improved function [31]. The effects of Kinesio Tape and endurance training in improving the quality of life of knee OA were compared for participants between the ages of 40-70 years, and both interventions were equally effective in improving the quality of life [32].Meta-analysis recruited participants of knee OA and found that conventional therapy and circuit training showed improvement in knee stiffness, activities of daily living, and quality of life [33]. Similar findings are also achieved in our study in which elliptical training and conventional therapy showed significant improvement in knee outcomes. Knee Joint Mobilization generates rhythmic oscillatory movements within the normal joint range. Joint mobilization reduced pro-inflammatory gene activation (e.g., IL-1β, cyclooxygenase, etc), leading to improved local inflammation, reduction in pain, and improvement in knee ROM.
Due to the limited resources this study was done at a low-cost budget. Follow-up was of a short period with a small sample size that may limit the generalizability of results. To provide a comprehensive understanding of the lasting effects, a longitudinal follow-up study should be conducted beyond 12 weeks. Future studies should investigate the use of sophisticated imaging techniques such as magnetic resonance imaging (MRI) and computed tomography (CT) scans to have precise information regarding joint structures, cartilage integrity, and knee spacing, providing a full assessment of the course of knee osteoarthritis (OA) by including diverse participants with large sample size to apply findings on the broader population. Future studies should compare elliptical training with other types of interventions as well to determine relative effectiveness as well.
CONCLUSION
As both groups improved in terms of the KOOS variables, elliptical exercise was found to be good for the relief of pain, stiffness, ADLs, sports, and QOL. Furthermore, post-x-rays of medial knee joint space width (JSW) showed favorable outcomes, indicating that elliptical training can be employed for interventional purposes in persons with grades 1 and 2 of osteoarthritis of the knee.
DECLARATIONS & STATEMENTS
Author’s Contribution
SSKB, AA and SR: substantial contributions to the conception and design of the study.
SSKB, SR: acquisition of data for the study.
SSKB, AA and ZA: analysis of the data for the study.
SSKB, ZA, SR: interpretation of data for the study.
SSKB: drafted the work.
SSKB, AA, SM, ZA and SR: revised it critically for important intellectual content.
SSKB, AA, SM, ZA and SR: final approval of the version to be published and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors contributed to the article and approved the submitted version.
Ethical Statement
The study was conducted at the Islamabad Physical Therapy and Rehabilitation Centre (IPRC-21-01-2022-23), Rawalpindi, Pakistan after approval was taken from the research and ethical committee (REC) of the Faculty of Rehabilitation and Allied Health Sciences (RIPHAH/RCRS/REC/Letter-01238) Riphah International University.
Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
None to declare.
Conflicts of Interest
The authors declare no conflict of interest.
Funding
None to declare.
REFERENCES
- Sajaan Almansour SH, Singh R, Hadrami Alyami SM, Sharma N, Reshan A, Saleh M, et al. A convolution neural network design for knee osteoarthritis diagnosis using x-ray images. Int. J. Online Biomed. Eng.. 2023;19(7). [CrossRef]
- Aseem S, Khanam FM, Ghori SH, Sufiyanuddin M, Yaseen MM. Incidence density and relative rate assessment of knee osteoarthritis with respect to BMI, age and gender conducted in a tertiary care hospital in Hyderabad, India. Int J Community Med Public Health. 2023;10(4):1502. [CrossRef]
- GABADA R, Telang P. Assistive and rehabilitation technology in osteoarthritis of knee. J. Pharm. Negat. Results. 2022:3027-30. [CrossRef]
- Pratama WF, Fuzianingsih EN. Body mass index and knee osteoarthritis: a retrospective cross-sectional study in baptis hospital, batu city. J. Ilm. Kedokt. Wijaya Kusuma 2023;12(1):84-91. [CrossRef]
- Cueva JH, Castillo D, Espinós-Morató H, Durán D, Díaz P, Lakshminarayanan V. Detection and classification of knee osteoarthritis. Diagnostics (Basel). 2022;12(10):2362. [CrossRef] [PubMed]
- Hayes B, Kittelson A, Loyd B, Wellsandt E, Flug J, Stevens-Lapsley J. Assessing radiographic knee osteoarthritis: an online training tutorial for the Kellgren-Lawrence Grading Scale. MedEdPORTAL. 2016;12:10503. [CrossRef] [PubMed]
- Ji X, Ito A, Nakahata A, Nishitani K, Kuroki H, Aoyama T. Effects of in vivo cyclic compressive loading on the distribution of local Col2 and superficial lubricin in rat knee cartilage. J Orthop Res . 2021;39(3):543-52. [CrossRef] [PubMed]
- 8. Hummer E, Murphy E, Suprak DN, Brilla L, San Juan JG. The effects of a standard elliptical vs. a modified elliptical with a converging footpath on lower limb kinematics and muscle activity. J Sports Sci . 2020;38(20):2382-9. [CrossRef] [PubMed]
- Arifin Z, Prasetyo SD, Suyitno S, Tjahjana DDDP, Rachmanto RA, Juwana WE, et al. Rancang bangun alat elliptical trainer outdoor. Mekanika: Majalah Ilmiah Mekanika. 2020;19(2):104-12.
- Hasebe Y, Akasaka K, Otsudo T, Hall T, Yamamoto M. Effects of incorporating elliptical trainer exercise during rehabilitation on physical function and self-reported outcomes after total hip arthroplasty: a randomized controlled trial. J Phys Ther Sci. 2022;34(3):230-5. [CrossRef] [PubMed]
- Sade S, Pickholtz H, Melzer I, Shapiro A. Development of an elliptical perturbation system that provides unexpected perturbations during in-place walking (the epes system). J Neuroeng Rehabil. 2023. [CrossRef] [PubMed]
- Schirò S, Foreman S, Joseph G, Souza R, McCulloch C, Nevitt M, et al. Impact of different physical activity types on knee joint structural degeneration assessed with 3-T MRI in overweight and obese subjects: data from the osteoarthritis initiative. Skeletal Radiol . 2021;50:1427-40. [CrossRef] [PubMed]
- Larsen P, Rathleff MS, Roos EM, Elsoe R. Knee injury and osteoarthritis outcome score (KOOS)–National record-based reference values. Knee. 2023;43:144-52. [CrossRef] [PubMed]
- Kim J-H, Min Y-K, Jang Y-C, Seo W-S. Serial changes of fatty degeneration and clinical outcomes after repair of medium-sized rotator cuff tears. Clin Orthop Surg. 2024;16(1):95. [CrossRef] [PubMed]
- Robotti E, Leone F. Reply: Cone-Beam Computed Tomography: A user-friendly, practical roadmap to the planning and execution of every rhinoplasty—a 5-year review. Plast Reconstr Surg. 2022;150(3):697e-8e. [CrossRef] [PubMed]
- Gürkan G, Atar M, GÜRKAN G. Importance of preoperative vertical geometric analysis in surgery for anterior communicating artery aneurysm. Cureus. 2023;15(7). [CrossRef] [PubMed]
- Leung K, Zhang B, Tan J, Shen Y, Geras KJ, Babb JS, et al. Prediction of total knee replacement and diagnosis of osteoarthritis by using deep learning on knee radiographs: data from the osteoarthritis initiative. Radiology. 2020;296(3):584-93. [CrossRef] [PubMed]
- Tsai L-C, Lee SJ, Yang AJ, Ren Y, Press JM, Zhang L-Q. Effects of off-axis elliptical training on reducing pain and improving knee function in individuals with patellofemoral pain. Controlled Clinical Trial. 2015;25(6):487-93. [CrossRef] [PubMed]
- Hummer ET, Murphy EN, Suprak DN, Brilla LR, San Juan JG. Movement direction impacts knee joint kinematics during elliptical exercise at varying incline angles. Knee. 2021;29:201-7. [CrossRef] [PubMed]
- Bricca A, Juhl CB, Steultjens M, Wirth W, Roos EM. Impact of exercise on articular cartilage in people at risk of, or with established, knee osteoarthritis: a systematic review of randomised controlled trials. Br J Sports Med. 2019;53(15):940-7. [CrossRef] [PubMed]
- Zheng L, Zhang Z, Sheng P, Mobasheri A. The role of metabolism in chondrocyte dysfunction and the progression of osteoarthritis. Ageing Res Rev. 2021;66:101249. [CrossRef] [PubMed]
- Martins D, Padavan D, Kahn A, Saum K, Rondon N, Litz AS, et al. Effects of impact versus non-impact cardiovascular machines in individuals between age 50 and 80 years. J. Popul. Ageing. 2020:1-13. [CrossRef]
- Coburn SL, Crossley KM, Kemp JL, Warden SJ, West TJ, Bruder AM, et al. Immediate and delayed effects of joint loading activities on knee and hip cartilage: a systematic review and meta-analysis. Sports Med Open. 2023;9(1):56. [CrossRef] [PubMed].
- Orekhov G, Robinson AM, Hazelwood SJ, Klisch SM. Knee joint biomechanics in transtibial amputees in gait, cycling, and elliptical training. PLoS One. 2019;14(12):e0226060. [CrossRef]
- Raposo F, Ramos M, Lúcia Cruz A. Effects of exercise on knee osteoarthritis: A systematic review. Musculoskeletal care. 2021;19(4):399-435. [CrossRef] [PubMed]
- Li S, Ng WH, Abujaber S, Shaharudin S. Effects of resistance training on gait velocity and knee adduction moment in knee osteoarthritis patients: a systematic review and meta-analysis. Sci Rep . 2021;11(1):16104. [CrossRef] [PubMed]
- Trams E, Kulinski K, Kozar-Kaminska K, Pomianowski S, Kaminski R. The clinical use of platelet-rich plasma in knee disorders and surgery—a systematic review and meta-analysis. Life (Basel). 2020;10(6):94. [CrossRef] [PubMed]
- Primorac D, Molnar V, Rod E, Jeleč Ž, Čukelj F, Matišić V, et al. Knee osteoarthritis: a review of pathogenesis and state-of-the-art non-operative therapeutic considerations. Genes (Basel) 2020;11(8):854. [CrossRef] [PubMed]
- Arshad N, Gondal MJI, Qamar MM, Basharat A. Manual therapy can be a potential therapy in knee osteoarthritis. Saudi J. Sports Med. 2018;18(1):18-21. [CrossRef] [PubMed]
- Sherazi F, Waqar S, Khalid M, Saleem K, Kiani SK, Shahzad M. Effect of knee joint mobilization on hamstring muscle length in patient with knee osteoarthritis. T. Rehabili. J. 2022;6(04):468-73. [CrossRef]
- Romanowski MW, Špiritović M, Romanowski W, Straburzyńska-Lupa A. Manual therapy (postisometric relaxation and joint mobilization) in knee pain and function experienced by patients with rheumatoid arthritis: a randomized clinical pilot study. Evid Based Complement Alternat Med . 2020;2020. [CrossRef] [PubMed]
- Nosheen I, Tahreem S, Akbar A, Sairien S, Haq K, Talha M. Comparison of kinesio-tapping and endurance training in improving quality of life in knee osteoarthritis: kinesio-tapping and endurance training in improving quality of life. Pak J Med Sci. [CrossRef]
- Al-Mhanna SB, Mohamed M, Mohd Noor N, Aldhahi MI, Afolabi HA, Mutalub YB, et al., editors. Effects of circuit training on patients with knee osteoarthritis: a systematic review and meta-analysis. Healthcare (Basel).2022:MDPI.[CrossRef][PubMed]

Submitted
Accepted
Published
How to Cite
Issue
Section
License
Copyright (c) 2024 Syed Sabih Ul Konain Bukhari, Anam Aftab, Sonia Munir, Zahoor Ahmad, Saad Rauf

This work is licensed under a Creative Commons Attribution 4.0 International License.
Authors retain copyright and grant the journal right of first publication and allows others to share the work with an acknowledgment of the work’s authorship and initial publication in this journal. No use, distribution or reproduction is permitted which does not comply with these terms.