Association of physical activity and risk of cardiac disease among young adults
DOI:
https://doi.org/10.52567/trehabj.v8i03.81Keywords:
Cardiac diseases, physical activity, risk factorsAbstract
Background: Nowadays the level of physical activity is compromised among all, especially in young adults, which may contribute to early development risk of cardiac disease.
Objective: To determine the association of risk of cardiac disease with physical activity among young adults.
Methods: A cross-sectional study was conducted from January 2024 to April 2024 at Iqra National University, Peshawar after approval from the ethical committee. A total of n=102 undergraduate male and female students between the age of 18-24 years were included in the study. To determine the physical activity of the participants International Physical Activity Questionnaire - Short Form was used. To evaluate the risk of cardiac disease was observed according to the National Cholesterol Education Program.
Results: The mean age and BMI of the n=102 study participants were 23.22±3.4 years and 23.37±5kg/m2 respectively. The risk of cardiac disease was found in n=45(44.1%) while most of the participants (n=33) were moderately and (n=42) highly physically active with a mean METs score of 2881.51±2704.83. Physical activity (PA) is not significantly associated (p=0.44) with the risk of cardiac disease. However, gender showed a strong association (p<0.001) with the risk of cardiac disease among the participants. A total of n=24(88.8%) females had the risk, out of n=27, while n=21(28%) males had the risk of cardiac disease out of n=75 males.
Conclusion: The study concluded that physical activity had a non-significant relation with the risk of cardiac disease while in the case of gender females are more prone to have the risk of cardiac disease.
INTRODUCTION:
Physical activity (PA) is a modifiable risk factor for different health outcomes, including cardiac disease [1] The chronic conditions associated with physical activity can be reduced by engaging in PA of at least 1200 MET-min/week. [2, 3]. Among young adults, Sedentary habits, poor time management, academic stress, psychosocial challenges, etc, contribute to the decline in physical activity. Ultimately increased health risks, particularly cardiovascular issues [4]. Raised CVD risk is due to low physical activity, which increases the triglycerides, reduces the HDL cholesterol, and also raises the fasting blood sugar by reducing insulin sensitivity [5]. A study showed that decreasing PA levels among young adults leads to CVD risk [6].
Interventions targeting lifestyle modifications, including increased PA, are essential for young adults to reduce CVD risk and promote overall cardiovascular health. Thus, maintaining or increasing PA is vital for young adults to lower their risk of cardiac disease [7]. A nationwide cohort study conducted in Pakistan reported that reduced PA activity from high to low levels increased the risk of increased risk of CVD [6]. In another study on the Pakistani young population, low physical activity was one of the risk factors for CVDs [8]. Furthermore, leisure-time physical activity (LTPA) is also negatively associated with risk of CVD[9, 10].
Currently, given the rising incidence of CVD among younger populations in Pakistan, there is an urgent need for targeted research that examines the association between physical activity and the risk of cardiac disease within this demographic. This study aims to identify the current association between physical activity and the risk of cardiac disease among young adults in Pakistan.
METHODOLOGY
Study Design & Setting: This cross-sectional study was conducted from January 2024 to April 2024 at Iqra National University, Peshawar after approval from the ethical committee (IQN-EC:1102024). The data was collected according to the Declaration of Helsinki and prior to the study written informed consent was obtained. From the students and their parents.
Participants: Undergraduate male and female students between 18-24 years were included in the study. Those students with known metabolic, hormonal, and physical abnormalities were excluded.
Sample Size: A total n=108 sample size was calculated using the G*Power, with medium effect size (0.3), alpha (α) error probability 0.05, keeping the beta (β) error probability at 80% with 2 degrees of freedom(df). A total of n=160 were assessed for eligibility, n=52 students did not fulfill the inclusion criteria, while n=6 were excluded due to incomplete data. So final n=102 was analyzed.
Variables and outcome measures: The data was collected through a nonprobability convenient sampling technique. The demographic information was obtained as age, gender, and BMI. Moreover, to determine the physical activity of the participants International Physical Activity Questionnaire - Short Form was used. Their blood sample was taken for lipid profile, their 3 days dietary intake was taken to count their calorie intake, their waist circumference was taken, and physical activity was assessed through IPAQ to see results. To evaluate the risk of cardiac disease among young adults, waist circumference greater than 102 cm for men or greater than 88 cm for women; plasma triglycerides more than 150 mg/dl (1.7 mmol/L); HDL cholesterol more than 40 mg/dl (1.03 mmol/l) for men or less than 50 mg/dL (1.29 mmol/l) for women; blood pressure more than 130/85 mm Hg; and fasting plasma glucose more than 110 mg/dl (6.1 mmol/l). As per the National Cholesterol Education Programme, at least three of these requirements must be met [11].
Statistical methods: The Chi-square test of association was used to determine the relationship between Physical activity and risk of cardiac disease, as well as its association with gender. The demographic information was presented as mean, standard deviation, frequency, and percentages in tables and graphs. To determine the strength of association Phi & crammer was used, with the level of significance set at p<0.05. The SPSS version 23 was used for data analysis.
RESULTS
The mean age and BMI of the n=102 study participants were 23.22±3.4 years and 23.37±5kg/m2 respectively. A total of n=75 (73.5%) was male and the remaining n=27 (26.5%) were females. The descriptive statistics of the lipid profile are presented in Table 1.
Table 1: Descriptive statistics of lipid profile
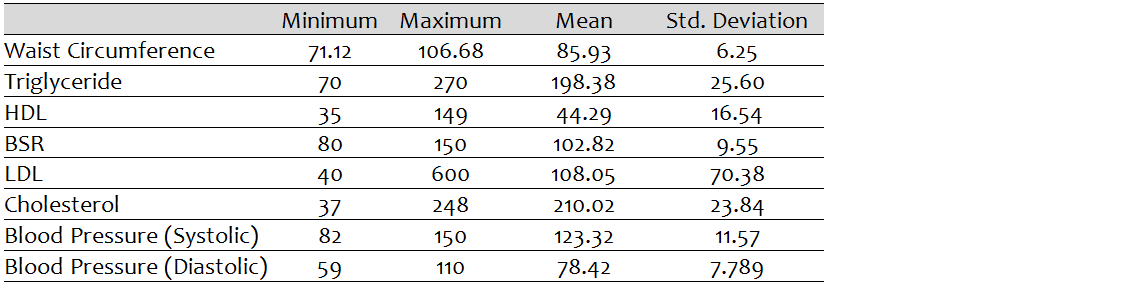
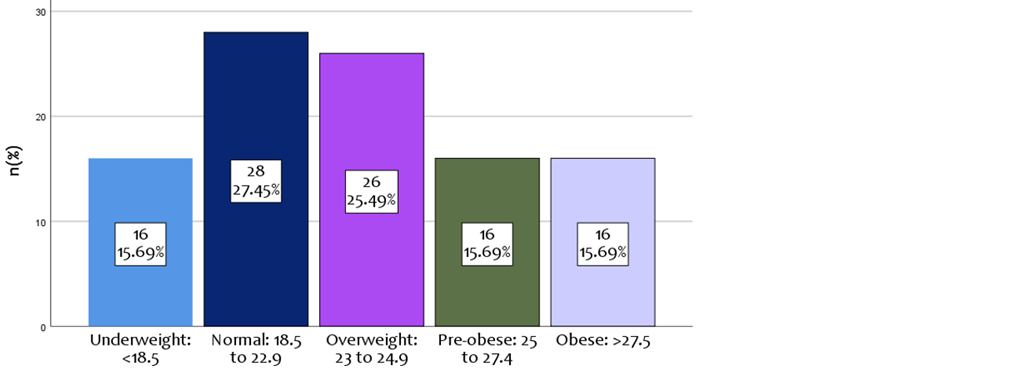
Figure 1: Frequency distribution of BMI
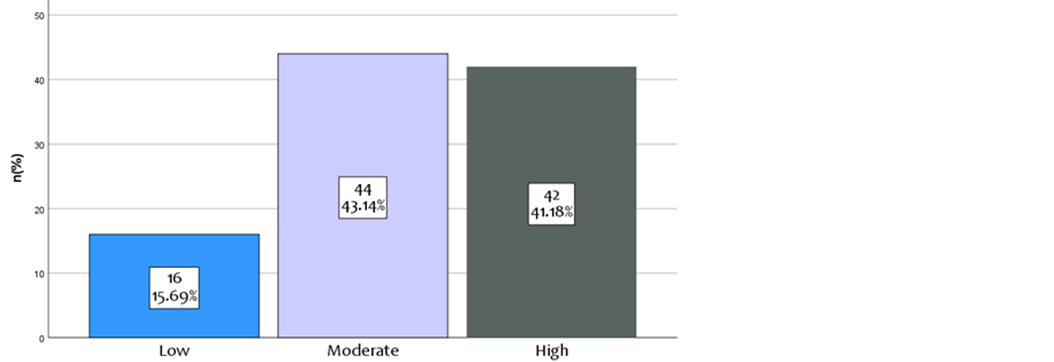
Figure 2: Frequency distribution of different levels of Physical Activity
Most participants were in the normal (n=28) and overweight (n=26) category of BMI respectively. (Figure 1) Regarding Physical activity level, most of the participants (n=33) were moderately and (n=42) highly physically active with a mean METs score of 2881.51±2704.83. (Figure 2)
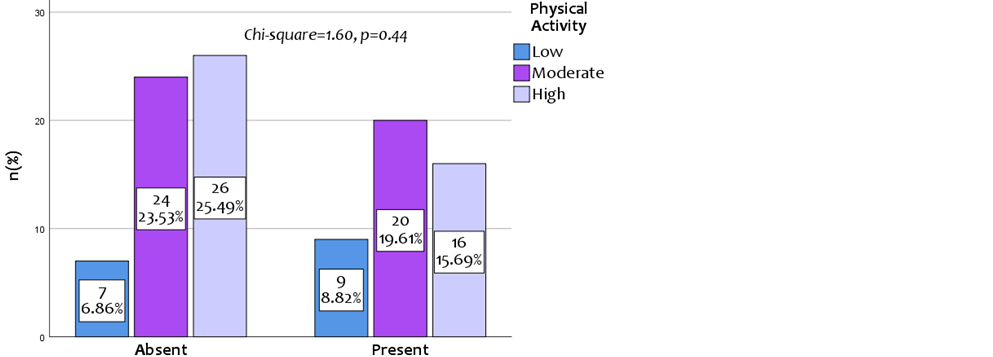
Figure 3: Association between physical activity and risk of cardiac disease
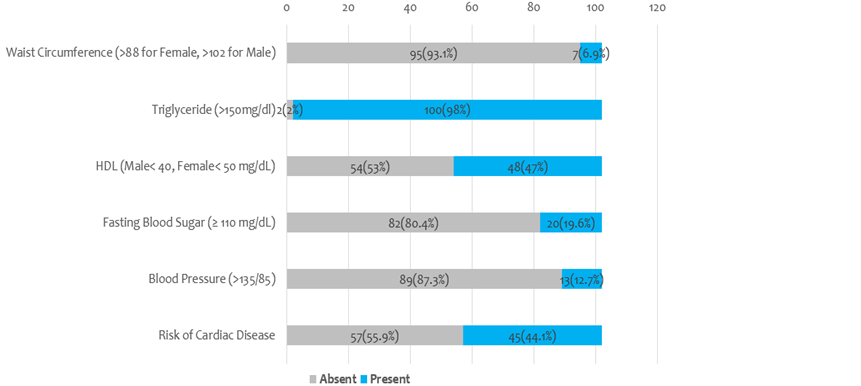
Figure 4: Frequency of risk of cardiac disease and individual factors among young adults
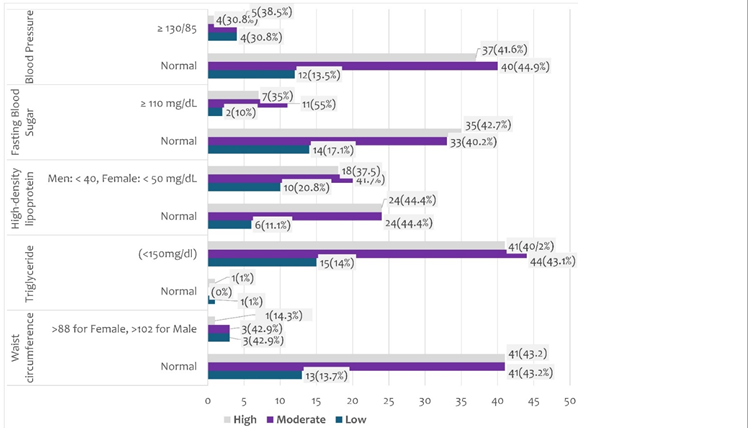
Figure 5: level of PA among individual factors contributing to the risk of cardiac disease
In Figure 3, the results showed that physical activity (PA) is not significantly associated (p=0.44) with the risk of cardiac disease. The frequency of risk of cardiac disease and individual factors among young adults is presented in Figure 4. Furthermore, the frequency of different levels of PA among the participants having risk of cardiac disease is n=9(8.82%) has low, n=20(19.6%) moderate, and n=16(15.69%) high PA. The detailed frequency distribution of different PA levels among individual factors contributes to the risk of cardiac disease (Figure 5) and PA is not significantly associated (p≥0.05) with any factor.
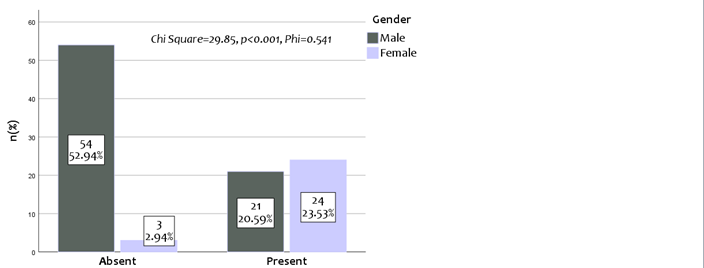
Figure 6: Association between gender and risk of cardiac disease
The result showed that the risk of cardiac disease was present among n=45(44.1%) participants out of n=102. Furthermore, Individual factors contributing to the risk are presented in Figure 5. It was observed that gender showed a strong association (p<0.001) with the risk of cardiac disease among the participants. A total of n=24(88.8%) females had the risk, out of n=27, while n=21(28%) males had the risk of cardiac disease out of n=75 males. (Figure 6)
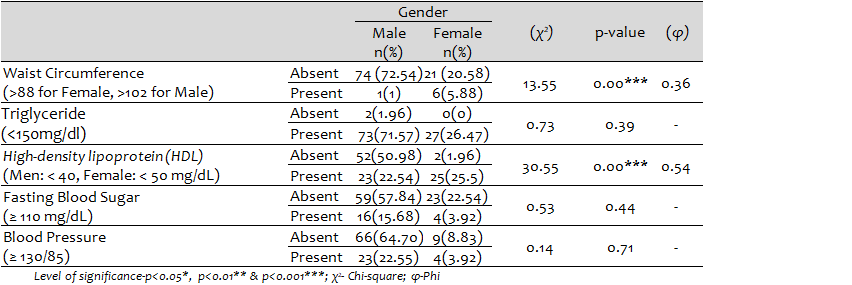
Regarding the factor contributing to the risk of cardiac disease, the results showed a very strong association of gender with waist circumference (χ2=13.55, p<0.001, φ=0.36) as well as with HDL (χ2=30.55, p<0.001, φ=0.54). While no significant association (p≥0.05) with triglyceride, fasting blood sugar, and blood pressure. When observing the frequency, out of n=75 male and n=21 female participants, n=1 male and n=6 female had greater waist circumference, HDL levels were found to be low in n=23 male and n=25 female, high fasting glucose levels in n=16 male and n=4 female and high blood pressure in n=23 male and n=4 female was observed. (table 2)
Table 2: Association of Gender and individual factors and Risk of Cardiac Disease
DISCUSSION
The objective of the study was to find association of physical activity (PA) and risk of cardiac disease (CD) among young adults. The results of the study showed that physical activity is non-significantly associated with risk of cardiac disease, but gender was significantly associated with risk of CD. Moreover, the risk of CD was highly prevalent in the female participants. Common factors were raised triglyceride levels and low levels of HDL in most participants. Females were more prone to have risk factors as compared to males.
However, in the current study physical activity is not significantly associated with the frequency of risk of cardiac disease. But numerous studies have revealed a link between physical inactivity and higher risks of coronary heart disease [12, 13]. Physical activity can lower the risk of cancer and cardiovascular disease by reducing dyslipidemia, hypertension, obesity, and glucose intolerance. The WHO recommended PA was linked to a decreased lifetime risk of CVD in both men and women when compared with a poor PA level[14].
Physical activity can lower the risk of cardiovascular disease by reducing dyslipidemia, hypertension, obesity, and glucose intolerance [15, 16]. The lack of a significant association between physical activity and cardiac disease risk in this study, despite most participants being moderately or highly physically active and 44% having cardiac disease risk, may be due to inaccuracies in assessing physical activity and risk factors. Self-reported physical activity data can be unreliable, leading to potential misclassification. Additionally, unmeasured confounding variables, such as a lack of baseline physical activity, dietary habits, smoking, genetic predisposition, or stress levels, may have masked the true relationship between physical activity and cardiac disease risk.
In the current study, the association between gender and the risk of cardiovascular disease (CVD) can be attributed to several lifestyle and dietary factors, even among participants who are moderately and highly physically active. Women generally exhibit a more favourable traditional CVD risk profile, yet they experience a higher relative risk from metabolic abnormalities like hyperglycemia and dyslipidemia compared to men [17]. Lifestyle-related factors such as high body mass index (BMI), high fasting blood glucose levels, and unhealthy dietary patterns (e.g., a mainly meat diet) significantly increase the risk of ischemic heart disease, with a more pronounced effect in women [18]. Additionally, while exercise is beneficial, the physiological responses to exercise can differ by sex, influencing cardiovascular remodelling and adaptation [19]. Furthermore, genetically increased low-density lipoprotein cholesterol (LDL-C) poses a greater risk for CVD in men than in women, suggesting that women may have different risk factor profiles that require tailored interventions [20]. Overall, lifestyle choices, dietary habits, and biological differences contribute to the gender disparities in cardiac disease risk [21].
The majority of the participants in the study had the risk factors of cardiac disease including high triglyceride levels, low HDL levels, raised blood pressure, raised fasting blood sugar level, and large waist circumference and more common in females. High triglyceride levels and low HDL cholesterol are often linked to lifestyle choices such as poor diet, physical inactivity, and obesity, which are prevalent in this age group [22, 23]. Additionally, the increasing incidence of metabolic syndrome, characterized by raised blood pressure and fasting blood sugar levels, is concerning, as it indicates a shift towards unhealthy physiological states in younger populations[24]. Gender differences also play a role, as studies show that young women may experience more pronounced cardiovascular adaptation issues, potentially due to hormonal influences and lifestyle factors [5]. Furthermore, the sedentary lifestyle and dietary habits, including high-fat diets, contribute significantly to these risk factors, emphasizing the need for targeted prevention strategies [25, 26].
The low sample size caused the young participants included with a skewed distribution of the physical activity in the data, which may cause a non-significant relationship.
CONCLUSION
The study concluded that physical activity had a non-significant relation with the risk of cardiac disease while in the case of gender females are more prone to have the risk of cardiac disease. Overall, this study emphasizes the need for gender[1]specific prevention strategies, particularly for females, and further research with larger, more diverse samples to better understand the relationship between PA and cardiac disease risk.
DECLARATIONS & STATEMENTS
Author’s Contribution
MB and MO: substantial contributions to the conception and design of the study.
MB, MO and AAS: acquisition of data for the study.
SI: analysis of the data for the study.
MB: interpretation of data for the study.
MB: drafted the work.
MB, MO, AAS, SI and MB: revised it critically for important intellectual content.
MB, MO, AAS, SI and MB: final approval of the version to be published and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors contributed to the article and approved the submitted version.
Ethical Statement
The study was conducted in Iqra National University, Peshawar from January 12 2024 to April 4 2024. Ethical approval was taken from Research Ethical Committee of Iqra National University, Peshawar.
Consent Statement
The written informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data is not publicly available due to privacy.
Acknowledgments
Thanks to the participants of this study for sharing their personal experience.
Conflicts of Interest
The authors declare no conflict of interest.
Funding
This research received no funding.
REFERENCES
- Nagata JM, Vittinghoff E, Gabriel KP, Rana JS, Garber AK, Moran AE, et al. Physical activity from young adulthood to middle age and premature cardiovascular disease events: a 30-year population-based cohort study. Int J Behav Nutr Phys Act. 2022;19(1):123. [CrossRef] [PubMed]
- López Sánchez GF, Mendiola Olivares J, Torres Cantero AM. Association between Physical Activity and 32 Chronic Conditions among Spanish Adults. Int J Environ Res Public Health. 2022;19(20). [CrossRef] [PubMed]
- Elagizi A, Kachur S, Carbone S, Lavie CJ, Blair SN. A Review of Obesity, Physical Activity, and Cardiovascular Disease. Curr Obes Rep. 2020;9(4):571-81. [CrossRef] [PubMed]
- Bélanger M, Casey M, Cormier M, Laflamme Filion A, Martin G, Aubut S, et al. Maintenance and decline of physical activity during adolescence: insights from a qualitative study. International Journal of Behavioral Nutrition and Physical Activity. 2011;8(1):117. doi: 10.1186/1479-5868-8-117. [CrossRef] [PubMed]
- Lee HR, Kim JK, Kim JH, Chung TH. Compared to serum triglyceride alone, the association between serum triglyceride to high-density lipoprotein cholesterol ratio and 10-year cardiovascular disease risk as determined by Framingham risk scores in a large Korean cohort. Clin Chim Acta. 2021;520:29-33. [CrossRef] [PubMed]
- Kim SR, Choi S, Kim K, Chang J, Kim SM, Cho Y, et al. Association of the combined effects of air pollution and changes in physical activity with cardiovascular disease in young adults. Eur Heart J 2021;42(25):2487-97. [CrossRef] [PubMed]
- Tran DT, Sojobi A. Review of the Scientific Literature on Young Adults Related to Cardiovascular Disease Intervention. Asian Pac Isl Nurs J. 2020;5(1):35-46. [CrossRef] [PubMed]
- Saleem M, Durrani AK, Adeeb M, Siddique AR. Psychosocial risk factors of cardiovascular disease in Pakistani adolescents and young adults: A Systematic Review. J Pak Med Assoc. 2020;70(9):1601-4. [CrossRef] [PubMed]
- Li J, Zhang Z, Si S, Xue FJFiCM. Leisure-time physical activity and cardiovascular disease risk among hypertensive patients: a longitudinal cohort study. 2021;8:644573. [CrossRef] [PubMed]
- Kamal AK, Khalid W, Zulfiqar M, Muqeet A, Zaidi F, Gowani A, et al. The potential of m-Health-based interventions to improve medication literacy and adherence in non-communicable diseases in Pakistan. 2019;14(3):NP8-NP10. [CrossRef] [PubMed]
- Lorenzo C, Williams K, Hunt KJ, Haffner SM. The National Cholesterol Education Program–Adult Treatment Panel III, International Diabetes Federation, and World Health Organization definitions of the metabolic syndrome as predictors of incident cardiovascular disease and diabetes. Diabetes care. 2007;30(1):8-13. [CrossRef] [PubMed]
- Peter-Marske KM, Evenson KR, Moore CC, Cuthbertson CC, Howard AG, Shiroma EJ, et al. Association of Accelerometer-Measured Physical Activity and Sedentary Behavior With Incident Cardiovascular Disease, Myocardial Infarction, and Ischemic Stroke: The Women's Health Study. J Am Heart Assoc. 2023;12(7):e028180. [CrossRef] [PubMed]
- Bendor CD, Bardugo A, Pinhas-Hamiel O, Afek A, Twig G. Cardiovascular morbidity, diabetes and cancer risk among children and adolescents with severe obesity. Cardiovasc Diabetol. 2020;19(1):79. [CrossRef] [PubMed]
- Kubota Y, Evenson KR, Maclehose RF, Roetker NS, Joshu CE, Folsom AR. Physical Activity and Lifetime Risk of Cardiovascular Disease and Cancer. Med Sci Sports Exerc. 2017;49(8):1599-605. [CrossRef] [PubMed]
- Masenga SK, Kirabo A. Hypertensive heart disease: risk factors, complications and mechanisms. Front Cardiovasc Med. 2023 Jun. [CrossRef] [PubMed]
- Kraus WE, Powell KE, Haskell WL, Janz KF, Campbell WW, Jakicic JM, et al. Physical activity, all-cause and cardiovascular mortality, and cardiovascular disease. Med Sci Sports Exerc.. 2019;51(6):1270. [CrossRef] [PubMed]
- Fappi A, Mittendorfer B. Different physiological mechanisms underlie an adverse cardiovascular disease risk profile in men and women. Proc Nutr Soc. 2020;79(2):210-8.. [CrossRef] [PubMed]
- Shin J, Ham D, Shin S, Choi SK, Paik HY, Joung H. Effects of lifestyle-related factors on ischemic heart disease according to body mass index and fasting blood glucose levels in Korean adults. PLoS One. 2019;14(5):e0216534. [CrossRef] [PubMed]
- Islam RA, Khalsa SSS, Vyas AK, Rahimian R. Sex-Specific Impacts of Exercise on Cardiovascular Remodeling. J Clin Med. 2021;10(17). [CrossRef] [PubMed]
- Cupido AJ, Asselbergs FW, Schmidt AF, Hovingh GK. Low-Density Lipoprotein Cholesterol Attributable Cardiovascular Disease Risk Is Sex Specific. J Am Heart Assoc. 2022;11(12):e024248. [CrossRef] [PubMed]
- Tokgozoglu L, Hekimsoy V, Costabile G, Calabrese I, Riccardi G. Diet, Lifestyle, Smoking. Handb Exp Pharmacol. 2022;270:3-24. [CrossRef] [PubMed]
- Uzokov J. Influence of abnormal lipid components in statin-naive young adults: Is there any gap? Eur J Prev Cardiol. 2020;27(8):868-9. [CrossRef] [PubMed]
- Siagian SN, Christianto C, Angellia P, Holiyono HI. The Risk Factors of Acute Coronary Syndrome in Young Women: A Systematic Review and Meta-Analysis. Curr Cardiol Rev. 2023;19(3): [CrossRef] [PubMed]
- Bhosale VV, Singh S, Srivastava M, Pathak P, Prakash S, Sonkar S, et al. A case control study of clinical and biochemical parameters of metabolic syndrome with special attention among young and middle aged population. Diabetes Metab Syndr. 2019;13(4):2653-9. [CrossRef] [PubMed]
- Kassam N, Ngunga M, Varwani M, Msunza M, Jeilan M. Acute coronary syndrome patterns in the Young: risk factor profile and in-hospital outcomes in a tertiary referral hospital in Kenya. BMC Cardiovasc Disord. 2024;24(1):192. [CrossRef] [PubMed]
- Abdullah Marzoog B. Adaptive and Compensatory Mechanisms of the Cardiovascular System and Disease Risk Factors in Young Males and Females. New Emir. Med. J. 2023;4(1):1-8. [CrossRef]

Submitted
Accepted
Published
How to Cite
Issue
Section
License
Copyright (c) 2024 Malaika Bano, Mian Omar

This work is licensed under a Creative Commons Attribution 4.0 International License.
Authors retain copyright and grant the journal right of first publication and allows others to share the work with an acknowledgment of the work’s authorship and initial publication in this journal. No use, distribution or reproduction is permitted which does not comply with these terms.