Effects of high intensity interval training on mobility and fitness outcomes in stroke
DOI:
https://doi.org/10.52567/trehabj.v8i04.75Abstract
Background: Stroke causes severe impairments in mobility, balance, and quality of life, making it the leading cause of disability globally. New research indicates that high-intensity interval training (HIIT) may benefit stroke patients more.
Objective: To determine the effects of high-intensity interval training on mobility and fitness outcomes in stroke.
Methods: A single-blinded, randomized controlled study was carried out on n=44 ambulatory stroke survivors between the ages of 45 and 65 years. The participants were randomly assigned to group A (n=22) received conventional physiotherapy (CPT). While Group B received HIIT in addition to conventional physiotherapy. The Berg Balance Scale (BBS), Heart Rate Recovery (HRR), Functional Ambulation Categories (FAC), Stroke-Specific Quality of Life (SS-QOL), Timed Up and Go (TUG) test, and the 6-Minute Walk Test (6MWT) were the outcome measures. At baseline, six weeks, and twelve weeks, assessments were carried out.
Results: The HIIT group had significantly improved mobility, balance, and cardiovascular fitness. In the 6MWT (p<0.001), BBS (p<0.001), FAC (p=0.002,), insignificant p-value in HRR (p=0.93, ηp²=0.00), SS-QOL (p=0.01, ηp²=0.16), and TUG tests (p=0.01, ηp²=0.16), and hence was better (p < 0.05) in all variables except FAC (0.48).
Conclusion: High-intensity interval Training significantly improves walking capacity, balance, cardiovascular recovery, and quality of life in stroke survivors when combined with conventional standard physiotherapy interventions, as compared to conventional physiotherapy alone.
INTRODUCTION
Stroke is a neurological condition caused lack of oxygen reaching the brain's areas leading to disability [1, 2]. Stroke ranks third in terms of contributing more to disability and is thought to be the second leading cause of death globally [3]. An ischemic stroke occurs when blood flow to the brain diminishes due to obstructions in vessels.[4].
Following a stroke, many patients face major physical impairments, such as walking, balance, coordination, and movement. These limitations can make simple chores like dressing, cooking, or moving across a room seem overwhelming and challenging [5]. Physical rehabilitation is critical to improve these abilities and recover independence, but for some survivors, these deficits might last for a long time, depending on the severity of the stroke and the parts of the brain affected[6, 7]. However, compared to healthy people, stroke survivors have half the cardiorespiratory fitness and nearly twice the energy costs for locomotion, which significantly increases their inactivity [8].
Systematic reviews indicate that focused interventions, including aerobic and strength training, can alleviate these challenges, improve functional capabilities, and elevate overall quality of life [9, 10, 11]. Generally, to increase cardiorespiratory fitness after a stroke moderate-intensity continuous cardiovascular exercise is advised [12]. Recent systematic reviews suggest that higher-intensity training, with a heart rate reserve of 60% or more, may be more effective for enhancing walking capacity and overall recovery [4]. High-intensity interval training has surfaced as a beneficial method for individuals experiencing neurological gait impairments, including those caused by conditions such as cerebral palsy or stroke [5]. The HIIT training method consists of alternating intervals of maximum speed walking followed by recovery periods, enabling patients to maintain elevated aerobic intensities in comparison to traditional continuous training [13].
The high-intensity exercises improve CRF, gait, and balance among stroke survivors; however, further research is needed to standardize protocols for long-term rehabilitation effects [14]. The rationale for incorporating HIIT into stroke rehabilitation stems from its potential to enhance cardiorespiratory fitness, improve mobility, and support cognitive recovery. As research continues to evolve, HIIT may become a cornerstone of rehabilitation protocols for stroke survivors, offering a time-efficient and effective approach to improving overall health outcomes. So, the objective was to evaluate the Effects of high-intensity interval training on mobility and fitness outcomes in stroke.
METHODOLOGY
Study Design and Setting: Single-blinded parallel two-group randomized controlled trial. Protocols were followed 3-5 days a week and 10-12 sets were performed one time a day for 12 weeks. The study was conducted with ethical approval (RIRAHS-ISB/REC/MS-PT/01745) and permission (RIPHAH/FR&AHS/Letter 014310) at Capital Hospital Islamabad, Grace Medical Centre, and IAT Aesthetic and Therapy.
Selection Criteria: The sample was collected through a nonprobability convenient sampling technique. This study comprised adult stroke survivors (aged 45–65) who were ambulatory and able to walk without help. This participant with co-morbid conditions such as cardiovascular disease, asthma/COPD, uncontrolled hypertension, and uncontrolled diabetes, as well as those with impaired cognition with a Mini-Mental State Examination (MMSE) score of more than 24, were excluded.
Sample size: the sample size of n=44 subjects was calculated Using G*Power, the sample size was determined with an alpha error probability of (α=0.05), an effect size of 0.25, and a power (1 – β) of 0.95. After the allocation into groups A and B. A total of n=49 subjects were evaluated for eligibility criteria, and n=5 declined participation due to not meeting the selection criteria (n=2) and accessibility issues (n=3). The remaining n=44 was randomly allocated equally to Groups A (n=22) and B (n=22). During the follow up there was n=08 loss of follow-up in groups A (n=4) and B (n=4). So in the data analysis, n= 36 participants were included. (Figure 1)
Randomization & Blinding: Sequentially numbered, opaque, sealed envelopes were used to hide the allocation of people into HIIT and conventional physical therapy groups. After recruiting and baseline evaluation, the envelopes were unsealed, and the treating therapists were given the information about randomization. This study is single-blinded because only the examiner knows about the intervention and group allocation the participants are not aware of groups.
The participants were randomly assigned to group A and received conventional physiotherapy (CPT). While Group B received HIIT in addition to CPT. Both interventions aimed at improving mobility and fitness in individuals with chronic stroke. HIIT Protocol: The HIIT protocol focuses on improving cardiovascular fitness, balance, and functional mobility through short, high-intensity exercises with rest intervals. Exercises included seated and standing balance, dynamic tasks, walking, and stationary cycling. Intensity ranged from 50-70% HR max, with progressive increases in duration (4–6 minutes) and complexity over 12 weeks, performed 5 days per week.
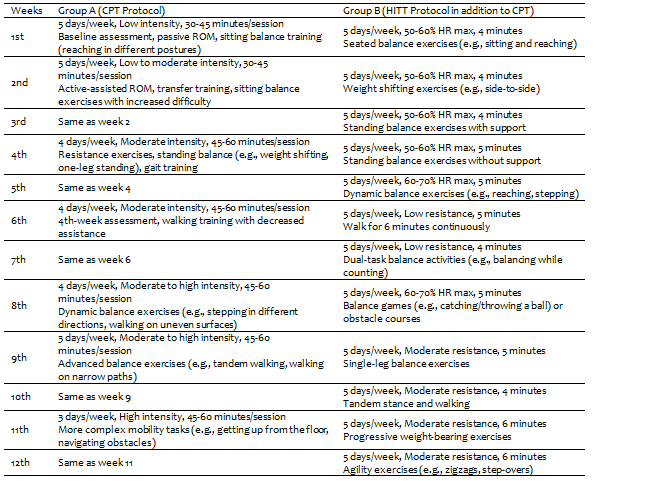
CPT Protocol: The CPT protocol followed traditional stroke rehabilitation, emphasizing balance, mobility, and strength. It included passive/active ROM exercises, sitting/standing balance, resistance training, and gait tasks. Sessions progressed in intensity (low to high) and duration (30–60 minutes) over 12 weeks, conducted 3–5 days per week. Further week-wise detail of the intervention in both groups has been presented in table 1.
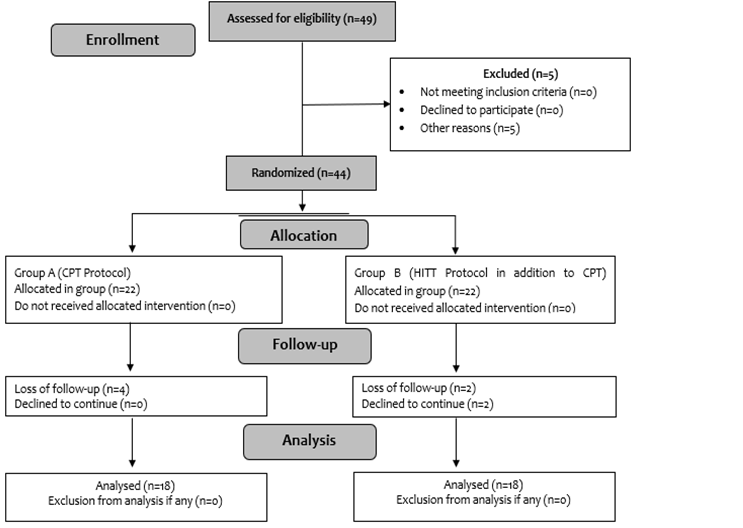
Figure 1: CONSORT flow diagram
Outcome Measure: The Six-Minute Walk Test (6MWT) is a validated and reliable assessment for stroke patients, measuring the distance they can walk in six minutes, which reflects their aerobic capacity and endurance[15]. Similarly, the Functional Ambulation Categories (FAC) scale evaluates the level of human support required for walking, using a 6-point scale from 0 to 5, and is effective in assessing mobility in stroke patients, requiring minimal space and equipment[16]. The Timed Up and Go Test (TUGT) assesses functional mobility by timing how long it takes a person to rise from a seated position, walk 3 meters, turn around, return, and sit down, serving as an indicator of fall risk and balance improvement[17]. The Berg Balance Scale (BBS) is another reliable tool that evaluates both static and dynamic balance through 14 tasks scored on a 4-point scale, although it does not assess gait[18]. Lastly, the Stroke Specific Quality of Life (SS-QOL) measure includes 12 domains assessing various aspects of life quality post-stroke, rated on a 5-point Likert scale, with higher scores indicating better quality of life[19]. All variables were measured at baseline, 6th week and 12th weeks.
Data analysis: Data was analyzed using SPSS version 21. Mixed ANOVA was applied for the interaction effects between treatment and level of assessment; 6MWT, FAC, TUGT, BBS, and SS-QOL. For main effects, the repeated measured ANOVA was applied with pairwise comparison, while for between-group comparison way, ANOVA was used with their effect size partial eta square (ηp2).
Table 1: Detailed description of Interventions of Group A (CPT) and Group B (CPT+HITT)
RESULTS
The age of the participants was 55.23±6.034 years. A total population of 44 was included in this study, of which 32 were males (69.6%) and 12 (26.1%) were females.
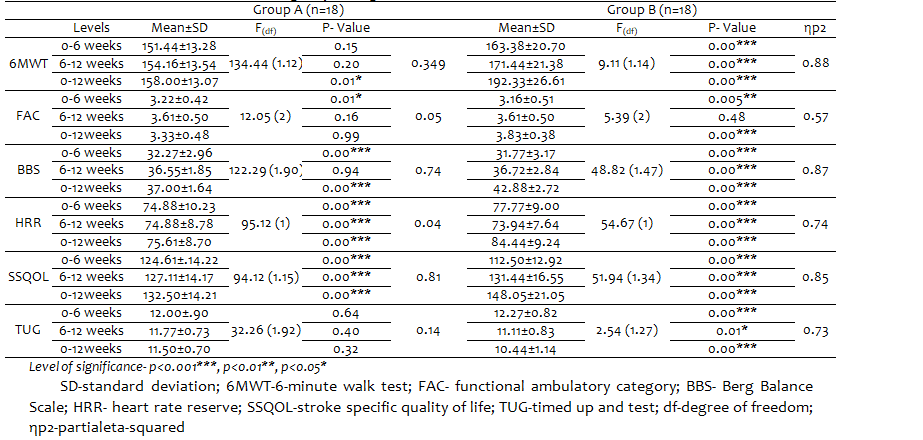
Mixed ANOVA showed that there was significant interaction effect observed in 6MWT {F(1.36, 123) =116, p=<0.001}, BBS {F(2, 21)=57.54, p<0.001}, FAC{ F(2, 54)=4.39, p<0.001}, HRR{ F(1.82, 314)=24.47, p<0.001}, SSQOL{ F(90.2, 156)=86.51, p<0.001 } and TUG{ F(1.82, 241,)=8.40, p<0.001}.
For within group changes RMANOVA was applied. The RMANOVA was used with pairwise comparison to determine the within-group Changes. In group A 6-MWT was significantly improved (p=0.01) from baseline to 12th week, But in pairwise comparison, no significant (p≥0.05) improvement was observed in 0-6 weeks and 6-12 weeks. When observing FAC, there was no overall significant improvement, but only in the initial 6 weeks results significantly (p=0.01) improved. The BSS also showed novel significant (p<0.001) improvement, while in pair-wise comparison, BBS improved significantly (p<0.001) only in the initial 6 weeks. The scores of HRR and SSQOL were significantly improved (p<0.001) overall as well as at each level of assessment till the 12th week. The TUG test was not Improved significantly (p≥0.05) . In group B, which received the HITT protocol in addition to CPT, Significant improvement (p<0.001) in all variables was observed from baseline to end of the 12th week as well as at each assessment level with a large effect size, except for FAC where from 6-12 week no significant (p=0.42) improvement observed. (Table 1)
The HIIT group showed significant improvements over the CPT group in most measures, especially after 12 weeks. Significant differences were seen in 6MWT, BBS, FAC, HRR, SSQOL, and TUG at the 12-week mark, indicating the effectiveness of the intervention on functional and quality-of-life outcomes.
Table 2: Within group changes in 6MWT, BBS, FAC, HRR, SSQOL, TUG
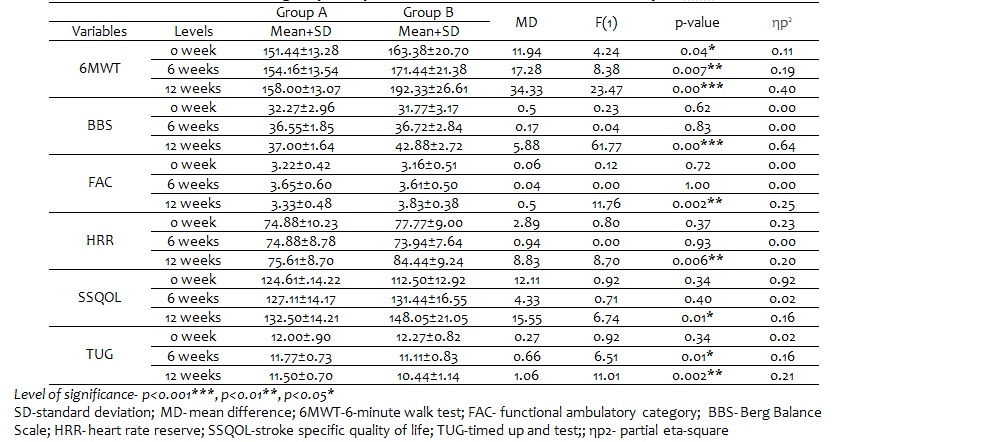
The One-way ANOVA showed significant improvement (p<0.05) in Group B received CPT and HIIT compared to Group A where only CPT was given in all variables after the 12th week. (Table 2)
As 6-MWT is not comparable at the baseline, the mean difference was compared which was 34. 33 after 12 weeks of intervention which shows marked improvement in mobility. The difference of 29.95 was observed in baseline and 12-week scores of 6MWT which are closer to a minimal clinically important difference in stroke subjects (34.4) in the HIIT group as compared to minimal change (6.56) in the control group.
Table 3: Between-group comparisons for 6MWT, BBS, FAC, HRR, SSQOL, TUG
DISCUSSION
This study found that high-intensity interval training (HIIT) significantly improved functional mobility, balance, endurance, and overall quality of life in stroke survivors. Over 12 weeks, participants in the group B who got HIIT in addition to conventional therapy outperformed group A, in several outcome measures.
Miller et al. (2019) observed that HIIT significantly enhanced walking capacity in stroke survivors, as analyzed by the 6-Minute Walk Test (6MWT), similar to the current study [20]. Both studies found an increase in walking distance, with the current study showing an average improvement of 18.54 meters, which is similar with Stoller et al.'s findings of a 20-meter increase. The similarity indicates that HIIT is helpful across a variety of sample sizes and stroke groups. Stoller et al. used a bigger sample size and a different HIIT methodology, focusing more on treadmill-based training, whereas the current study included both stationary cycling and walking physical activity. This difference in technique may have an impact on the precise processes that promote aerobic capacity and mobility.
In contrast, Boyne et al. observed no significant difference in balance results between HIIT and MICT for stroke recovery [21]. The difference may be due to differences in the duration and frequency of interventions. The current study used a 12-week program with 3-5 sessions per week, whereas Boyne et al. used a shorter 8-week intervention. Furthermore, Boyne et al. applied a lower intensity range for the HIIT procedure, which could have explained the absence of significant balance gains. In contrast, the current study found significant improvements in balance as viewed by the Berg Balance Scale (BBS), implying that higher-intensity training over a longer length of time may be essential for successful gains in postural stability [21].
This study's findings on functional mobility correlate with those of Dean et al. (2020), who observed that HIIT improved Timed Up and Go (TUG) scores more effectively than traditional rehabilitation methods [22]. Both studies reported significant decreases in TUG completion times, indicating increased functional mobility. However, Dean et al. focused on a more thorough neurological rehabilitation program that included cognitive activities in addition to HIIT, which may have influenced the extent of recovery [22]. In contrast, the current trial focused primarily on physical rehabilitation and produced significant functional benefits.
Boyne et al. concluded that stroke survivors who underwent HIIT observed similar improvements in Stroke-Specific Quality of Life (SS-QOL) scores [23]. Both studies found that improvements in mobility and endurance led to higher self-reported quality of life.
A significant similarity between the current study and the study by Mayo et al exists; is the steady enhancement of walking ability and functional mobility through the implementation of HIIT protocols, highlighting its potential as a successful technique for rehabilitation. However the differences in balance results between this study and others highlight how crucial intensity and duration are when creating HIIT programs. The necessity for standardized protocols in stroke rehabilitation is further demonstrated by the differences in target populations, intervention designs, and sample sizes [24].
Although the study tried to cover various aspects of fitness, still there is a need for a detailed exploration of fitness outcomes along with mobility outcomes in stroke. The need for objective outcomes and the development of prognosis and recovery predicted by those outcomes can be included in future studies. The effects of HIIT can be studied for longer duration along with retention effects.
CONCLUSIONS
The study concludes that the combination of HHIT with conventional therapy has significantly improved mobility, balance, and fitness outcomes as compared to conventional therapy alone in post-stroke subjects.
DECLARATIONS & STATEMENTS
Author’s Contribution
KK, YKB, AE, NS, and RM: substantial contributions to the conception and design of the study.
KK, AE and NS: acquisition of data for the study.
KK, YKB and AE: analysis of the data for the study.
KK, NS and RM: interpretation of data for the study.
KK: drafted the work.
KK, YKB, AE, NS, and RM: revised it critically for important intellectual content.
KK, YKB, AE, NS, and RM: final approval of the version to be published and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors contributed to the article and approved the submitted version.
Ethical Statement
The study was conducted with ethical approval (RIRAHS-ISB/REC/MS-PT/01745) and permission (RIPHAH/FR&AHS/Letter 014310) at Capital Hospital Islamabad, Grace Medical Centre, and IAT Aesthetic and Therapy after approval from the administrators.
Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
None to declare.
Conflicts of Interest
The authors declare no conflict of interest.
Funding
None to declare.
REFERENCES
- Kuriakose D, Xiao ZJIjoms. Pathophysiology and treatment of stroke: present status and future perspectives. Int. J. Mol. Sci. 2020;21(20):7609. [CrossRef]
- Lee SY, Im SH, Kim BR, Han EYJAjopm, rehabilitation. The effects of a motorized aquatic treadmill exercise program on muscle strength, cardiorespiratory fitness, and clinical function in subacute stroke patients: a randomized controlled pilot trial. Am J Phys Med Rehabil. 2018;97(8):533-40. [CrossRef][PubMed]
- Kim Y-M, Lee H-J, Lee J-SJKSoPM. The effect of action observation training with acoustic stimulation on balance and gait in stroke patients. J Korean Soc Phys Med. 2021;16(4):13-21. [CrossRef][PubMed]
- Miller CM. Stroke Epidemiology. In: Lapchak PA, Yang G-Y, editors. Translational Research in Stroke. Singapore: Springer Singapore; 2017. p. 41-9. [CrossRef]
- Mohammed S, Haidar J, Ayele BA, Yifru YM. Post-stroke limitations in daily activities: experience from a tertiary care hospital in Ethiopia. BMC Neurology. 2023;23(1):364. doi: 10.1186/s12883-023-03419-9. [CrossRef]
- Ramanathan S, Lynch E, Bernhardt J, Nilsson M, Cadilhac DA, Carey L, et al. Impact assessment of the centre for research excellence in stroke rehabilitation and brain recovery. Health Res Policy Syst. 2023;21(1):30. [CrossRef][PubMed]
- Chalos V, van der Ende NA, Lingsma HF, Mulder MJ, Venema E, Dijkland SA, et al. National institutes of health stroke scale: an alternative primary outcome measure for trials of acute treatment for ischemic stroke. Stroke. 2020;51(1):282-90. [CrossRef][PubMed]
- Wiener J, McIntyre A, Janssen S, Chow JT, Batey C, Teasell RJP. Effectiveness of high‐intensity interval training for fitness and mobility post stroke: A systematic review. PM R. 2019;11(8):868-78. [CrossRef][PubMed]
- Billinger SA, Arena R, Bernhardt J, Eng JJ, Franklin BA, Johnson CM, et al. Physical activity and exercise recommendations for stroke survivors: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(8):2532-53. [CrossRef][PubMed]
- Saunders D, Greig C, Young A, Mead G. Physical fitness training for stroke patients (Cochrane Review). The Cochrane Library. Cochrane Database Syst. 2004;(1). [CrossRef][PubMed]
- Teasell R, Mehta S, Pereira S, McIntyre A, Janzen S, Allen L, et al. Time to rethink long-term rehabilitation management of stroke patients. T Top Stroke Rehabil. 2012;19(6):457-62. [CrossRef][PubMed]
- Crozier J, Roig M, Eng JJ, MacKay-Lyons M, Fung J, Ploughman M, et al. High-intensity interval training after stroke: an opportunity to promote functional recovery, cardiovascular health, and neuroplasticity. Neurorehabil Neural Repair. 2018;32(6-7):543-56. [CrossRef][PubMed]
- Coates AM, Joyner MJ, Little JP, Jones AM, Gibala MJ. A perspective on high-intensity interval training for performance and health. Sports Med. 2023;53(Suppl 1):85-96. [CrossRef][PubMed]
- Baricich A, Borg MB, Battaglia M, Facciorusso S, Spina S, Invernizzi M, et al. High-intensity exercise training impact on cardiorespiratory fitness, gait ability, and balance in stroke survivors: a systematic review and meta-analysis. J Clin Med. 2024;13(18):5498. [CrossRef][PubMed]
- Agarwala P, Salzman SH. Six-Minute Walk Test: Clinical Role, Technique, Coding, and Reimbursement. Chest. 2020;157(3):603-11. [CrossRef][PubMed]
- Yoo YJ, Lim SH. Assessment of Lower Limb Motor Function, Ambulation, and Balance After Stroke. Brain Neurorehabil. 2022;15(2):e17. [CrossRef][PubMed]
- Ortega-Bastidas P, Gómez B, Aqueveque P, Luarte-Martínez S, Cano-de-la-Cuerda R. Instrumented Timed Up and Go Test (iTUG)-More Than Assessing Time to Predict Falls: A Systematic Review. Sensors (Basel). 2023;23(7). [CrossRef][PubMed]
- Miranda N, Tiu TK. Berg Balance Testing. StatPearls. Treasure Island (FL) ineligible companies. Disclosure: Timothy Tiu declares no relevant financial relationships with ineligible companies.: StatPearls Publishing. Copyright © 2024, StatPearls Publishing LLC.; 2024. [PubMed]
- Lin KC, Fu T, Wu CY, Hsieh CJ. Assessing the stroke-specific quality of life for outcome measurement in stroke rehabilitation: minimal detectable change and clinically important difference. Health Qual Life Outcomes. 2011;9:5. [CrossRef][PubMed]
- Miller A, Reisman DS, Billinger SA, Dunning K, Doren S, Ward J, et al. Moderate-intensity exercise versus high-intensity interval training to recover walking post-stroke: protocol for a randomized controlled trial. Trials. 2021;22:1-15. [CrossRef][PubMed]
- Boyne P, Billinger SA, Reisman DS, Awosika OO, Buckley S, Burson J, et al. A multicenter randomized comparison of high-intensity interval training and moderate-intensity exercise to recover walking post-stroke: Results of the HIT-stroke trial. medRxiv. 2022:2022.08. 01.22278246. [CrossRef]
- Dudley D, Weaver N, Cairney J. High-intensity interval training and health optimizing physical education: Achieving health and educative outcomes in secondary physical education—A pilot nonrandomized comparison trial. J Journal of Teaching in Physical Education. 2020;40(2):215-27. [CrossRef]
- Boyne P, Dunning K, Carl D, Gerson M, Khoury J, Rockwell B, et al. High-intensity interval training and moderate-intensity continuous training in ambulatory chronic stroke: feasibility study. Phys Ther. 2016;96(10):1533-44. [CrossRef][PubMed]
- Mayo NE, Anderson S, Barclay R, Cameron JI, Desrosiers J, Eng JJ, et al. Getting on with the rest of your life following stroke: a randomized trial of a complex intervention aimed at enhancing life participation post stroke. Clin Rehabil. 2015;29(12):1198-211. [CrossRef][PubMed]

Submitted
Accepted
Published
How to Cite
Issue
Section
License
Copyright (c) 2024 Kiran Khushnood, Yousaf Khan Burki, Aqsa Ejaz, Nasir Sultan, Riafat Mehmood

This work is licensed under a Creative Commons Attribution 4.0 International License.
Authors retain copyright and grant the journal right of first publication and allows others to share the work with an acknowledgment of the work’s authorship and initial publication in this journal. No use, distribution or reproduction is permitted which does not comply with these terms.