Effects of treadmill training on cardiorespiratory endurance and constipation in children with cerebral palsy: a randomized clinical trial
DOI:
https://doi.org/10.52567/trehabj.v10i01.145Keywords:
cerebral palsy, cardiorespiratory endurance, constipation, 6- minute walk test, physical therapy, treadmill trainingAbstract
Background: Children with cerebral palsy (CP) commonly experience reduced cardiorespiratory endurance due to limited mobility and sedentary lifestyle. Constipation is also a frequent comorbidity affecting their health and quality of life. Treadmill training has been suggested as an effective intervention to improve physical fitness and functional mobility in children with CP.
Objective: To evaluate the effects of treadmill training on cardiorespiratory endurance and constipation in children with spastic diplegic cerebral palsy.
Methodology: A randomized clinical trial was conducted from January to May 2024 at Rahman Medical Institute and Akbar Kare Institute, Peshawar. Thirty-six children with spastic diplegic CP (aged 4–10 years; GMFCS levels I–II) were randomly assigned to treadmill training plus conventional physical therapy (TT, n=18) or conventional physical therapy alone (CPT, n=18). The intervention lasted 12 weeks with progressive exercise intensity. Cardiorespiratory endurance was assessed using the 6-Minute Walk Test (6MWT), while constipation severity was measured using the Constipation Assessment Scale (CAS). Data were analyzed using MANOVA, independent t-test, and repeated-measures ANOVA (α≤0.05).
Results: MANOVA showed a significant overall effect of intervention on combined outcomes (Pillai's Trace=0.338, p=0.002). The TT group demonstrated significantly greater improvement in 6MWT distance compared with the CPT group (p<0.001). However, no significant between-group differences were observed for CAS scores (p=0.444), although both groups showed within-group improvement over time.
Conclusion: Treadmill training significantly improves cardiorespiratory endurance in children with spastic diplegic cerebral palsy but does not provide additional benefits for constipation compared with conventional therapy alone.
Clinical Trail # NCT06480448
INTRODUCTIONCerebral palsy (CP) is a neurodevelopmental disorder that affects motor functions, muscle tone, and posture[1]. It is often associated with various comorbidities, including cardiovascular issues and gastrointestinal problems such as constipation[2]. Physical therapy, particularly treadmill training, has been shown to improve these conditions by enhancing motor skills, cardiovascular fitness, and gastrointestinal function[3]. Purpose of this study is to assess how treadmill training affects children with cerebral palsy's cardiorespiratory endurance and constipation[4,5,6].
Cardiorespiratory endurance is the capacity of the circulatory and respiratory systems to provide working muscles with oxygen and nutrients during an extended duration of physical exercise, because of their restricted movement, stiffness, weak muscles, and sedentary lifestyles children with cerebral palsy (CP) usually have poor cardiorespiratory fitness[4,7]. Decreased cardiorespiratory endurance can worsen overall health, increases the risk of obesity, cardiovascular disease and respiratory dysfunction making it more difficult to perform physical activity[5,8].
Inpatient Constipation is a common gastrointestinal issue that affects up to 74% of children with cerebral palsy[6,9]. Changes in diet, medication, immobility, and neurological dysfunction are some of the many etiologies of constipation in individuals with cerebral palsy (CP). Constipation has a major impact on the general health, comfort, and quality of life of children with cerebral palsy (CP). If neglected, it may cause pain, discomfort, faecal impaction, faecal incontinence, and urinary system problems[10,11].
Treadmill training has demonstrated potential benefits as a therapeutic intervention for improving motor function, gait, and overall physical fitness. Participants in this intervention can walk on a motorized treadmill under the supervision of certified therapists[12,13]. Furthermore, aerobic exercise through treadmill training has been shown to improve cardiorespiratory endurance by 15% to 40% depending on the intensity and duration of the program[14]. The link between aerobic exercise and cardiovascular health is well-established, but there is limited but emerging evidence suggesting that increased mobility and physical therapy may also improve defecation frequency and constipation severity in children with CP[15].
Despite the known benefits of treadmill training for motor and aerobic outcomes, its potential impact on secondary autonomic functions like gastrointestinal motility remains insufficiently explored. Given that decreased mobility is a primary contributor to constipation in CP, it is hypothesized that the systematic physical activity provided by treadmill training may simultaneously enhance cardiorespiratory fitness and alleviates constipation symptoms. This study aims to evaluate the effects of a treadmill training program on cardiorespiratory endurance and constipation severity in children with cerebral palsy to provide a more holistic approach to their rehabilitation.
METHODOLOGYStudy design and setting
Randomized clinical trial was initiated after getting approval from the Research Ethic Committee (REC) of Riphah International University, Islamabad (Riphah/RCRANS-ISB/REC/MS-PT/01826). The study was conducted at Rahman Medical Institute (RMI)(RMI/30-11-2023) and Akbar Kare Institute (AKI) (AKI-PT/2023-12) Peshawar from Jan 2024 to May 2024. The individuals were told of the study's goal, and participants provided signed informed permission.
Selection criteria
A non-probability convenience sampling technique was employed for data collection. The children diagnosed with spastic diplegic cerebral palsy, aged between 04-10 years, having I or II level of dependency on GMFCS with intact cognitive abilities were included in the study. Moreover, the children with mental retardation, other neurological abnormalities, uncontrolled seizures, prior similar training, multiple contractures, and significant respiratory issues, use of muscle relaxants, and hearing or communication problems were excluded the research.
Randomization and Blinding
Participants who met the eligibility criteria were randomly allocated into treadmill training group (TT) and the conventional physical therapy group (CPT) in a 1:1 ratio. Randomization was performed using a computer-generated random allocation sequence to minimize selection bias. The allocation sequence was prepared prior to participant enrolment, and participants were assigned to groups accordingly. It was not possible to blind the therapists providing the treatment or the participants receiving the intervention. However, to reduce potential assessment bias, the outcome assessor was kept blinded to the group allocation of the participants during data collection for the 6-Minute Walk Test (6MWT) and Constipation Assessment Scale (CAS). Additionally, the data analysis was conducted without revealing the group identity, ensuring objective statistical evaluation. Therefore, the study followed a single-blinded randomized clinical design, where the outcome assessor and data analyst were blinded, while the therapists and participants were aware of the intervention being delivered.
Sample Size
A total of n=36 was calculated from G power, with an effect size of just 0.2 and an α error margin of 0.05. In order to mitigate the risk of β mistake, a power (1-β) of 0.95% was chosen. Total n=36 children diagnosed with spastic diplegic cerebral palsy were assessed for inclusion, it was found that n=16 people did not meet the selection requirements and were hence not included in the study. A total of n=36 individuals were split into groups A (18) and B (18) at random. A total n=52 participants screened, n=36 were randomized into control (n=18) and experimental (n=18) groups. Sixteen participants were excluded prior to randomization. During follow-up, two participants from the control group were lost, and one participant in the experimental group discontinued the intervention. Finally, n=16 participants in the control group and n=17 in the experimental group were analyzed for cardiorespiratory endurance and constipation outcomes.

Figure 1: CONSORT Diagram
Intervention Protocol
A 12-week structured intervention program was implemented, with participants assigned to either a treadmill training (TT) plus conventional physical therapy (CPT) group (Group A) or a CPT group (Group B). Both groups followed a progressive, phase-based protocol divided into three 4-week blocks (Weeks 1-4, 5-8, and 9-12), with exercise parameters adjusted at each stage to ensure appropriate progression.
Group A (Treadmill Training): In addition to CPT, the treadmill training protocol for Group A progressed in intensity and duration across the three phases. During the initial phase (Weeks 1-4), participants completed three sessions per week, each lasting 10 minutes at an intensity of 50-55% of age-predicted maximum heart rate (MHR) and a speed of 0.3 km/h. In the subsequent phase (Weeks 5-8), session frequency remained at three per week, but duration increased to 20 minutes, intensity was elevated to 55-60% MHR, and speed was increased to 1.0 km/h. During the final phase (Weeks 9-12), training frequency was increased to four sessions per week, with each session lasting 20 minutes at an intensity of 60-65% MHR and a speed of 3.0 km/h. to ensure the safety, support was provided by two trained physical therapists, one therapist stood behind the child and the other at the side, assisting in balance, posture correction during walk on treadmill. Participants were instructed to hold treadmill's parallel bars for added support. A visual feedback was provided by the mirror placed in front of the treadmill to encourage upright posture and correct gait mechanics. Verbal cues were also given throughout the sessions to guide and motivate the children.
Group B (Conventional Physical Therapy): The conventional therapy program for Group B consisted of a structured progression of therapeutic exercises across the three phases. In Weeks 1-4, participants performed core stability exercises, including supine bridging (10 repetitions, 2 sets), and stretching exercises targeting the hamstrings and calf muscles (10-second hold, 10 repetitions). During Weeks 5-8, the program advanced to weight-bearing exercises such as wall push-ups and standing balance activities (10 repetitions, 3 sets), in addition to balance and coordination training involving cone stepping and single-leg stance with support (10 repetitions, 3 sets). In the final phase (Weeks 9-12), participants engaged in strengthening exercises, including sit-to-stand and resistance band kicking (10 repetitions, 3 sets), gait training involving walking in parallel bars (5 minutes per session), and standing frame activities that required reaching for objects placed on a tray or table to encourage upper limb engagement and trunk control (5 minutes per session).
Outcome Measures
6-Minute Walk Test (6MWT): 6MWT was used to evaluate cardiorespiratory endurance in children with CP. By recording the distance walked in six minutes. The 6MWT showed good levels of validity while using with cerebral palsy children and it has a high degree of test retest reliability (ICC=0.98)[16].
Constipation Assessment Scale (CAS): CAS was used to assess the severity of constipation symptoms in CP children. the Constipation assessment scale showed good level of reliability (ICC=0.95)[17].
Statistical Analysis
SPSS version 28 was used to analyse the data. To determine the effects of interventions on combine dependent variables, MANOVA test was applied on mean change of endurance and constipation severity. As the significant effect observed, so for main effects, between the group differences were measured with independent t-test, and for within group changes EM ANOVA was applied. The level of significance was measured at alpha (α) <0.05. All tests was applied through SPSs ver 26.
There was n=36 participants having age of 7.06±1.55 years, the participants age varies from 4 to 9 years, suggesting a relatively young group with a limited age range scale. Out of the total sample, n=24 (64.9%) participants were male and n=12 (32.4%) participants were female, indicating a higher frequency of males in the study. The multivariate analysis of variance (MANOVA) on mean change, revealed a statistically significant overall effect of group on the combined dependent variables, Pillai's Trace=.338, F(2, 30)=7.672, p=.002, partial η²=.338, indicating a large effect size. This suggests that the type of intervention (CPT+TT vs. CPT) significantly influenced the overall outcome profile. Further univariate analyses showed a significant difference between groups for the Six-Minute Walk Test (Six MWT), F(1, 31)=15.807, p<0.001, partial η²=.338, with the CPT+TT group demonstrating higher mean walking distance (x̄=86.80) compared to the CPT group (x̄= 77.09). The effect size was large, indicating substantial clinical and statistical importance. In contrast, no significant group difference was observed for the Composite Assessment Scale (CAS), F(1, 31)=0.601, p=.444, partial η²=.019, suggesting a negligible effect. Overall, the findings indicate that the combined CPT+TT intervention significantly improves functional capacity (Six MWT), while it does not produce a meaningful difference in CAS scores compared to CPT alone.
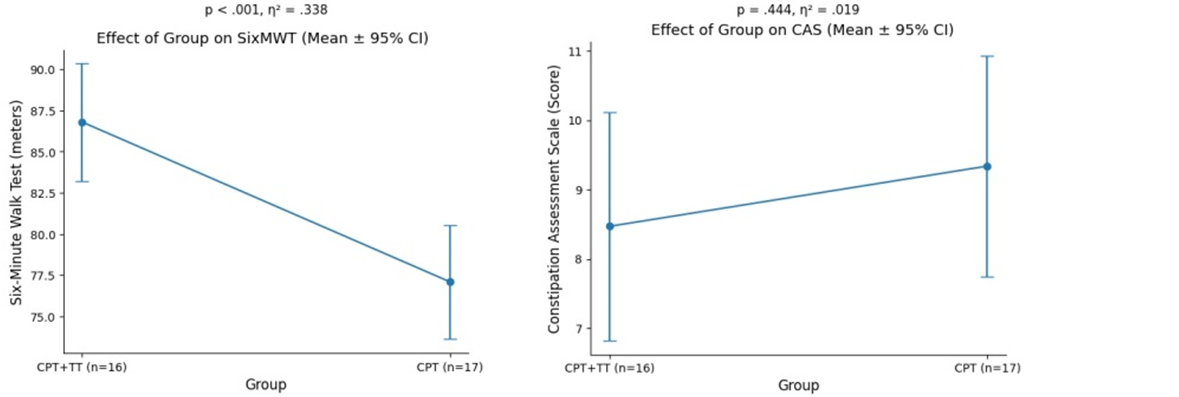
Figure 2: Effect of intervention on combine dependent variable (endurance & constipation)
At baseline, the TT group demonstrated significantly higher scores compared to the CPT group (p=0.027), indicating a statistically significant difference between groups at the start of the study. At the 4th week, the difference was not statistically significant (p=0.083). By the 8th week, the TT group showed marked significant improvement group (p<0.001) compared to the CPT. Similarly, at the 12th week, the TT group continued to improve significantly (p<0.001) than the CPT group. While both interventions reduced the CAS scores over time; however, no statistically significant (p≥0.05) difference between TT and CPT was observed for CAS outcomes.
Table 1: Between-group comparison (Independent T-test)

Within group changes with RM ANOVA, the both endurance and constipation were significantly improved from baseline to the twelfth week in the intervention group at each assessment level. While the endurance in the CPT group showed significant improvement (p<0.05) only from baseline to the 4th week, while no significant change from 4th to 8th week (p≥0.05), and from 8th to 12th week. Similarly, Constipation Assessment Scale (CAS) in the control group showed significant improvement only from baseline to the 4th week (p<0.01).
Table 2: Within-group analysis (repeated measure ANOVA)

In this study, treadmill training along with conventional physical therapy significantly the functional endurance with large effect size, as measured by the 6‑Minute Walk Test (6MWT). This finding is consistent with study, which shown that structured, progressive exercise protocols (often including treadmill walking) improve walking distance and fitness[18]. Tauro et al. (2024) also reported that a 12-week cardiovascular exercises improved children's 6MWT distance, improved VO₂ max and fatigue scores[19]. The present results also aligned with previous evidence that task-specific, repetitive gait training can substantially boost endurance and walking capacity in ambulatory CP children[20].
Treadmill walking provides a high-repetition, task-specific stimulus that trains both the cardiovascular system and the neuromuscular control of gait. Over 12 weeks, the protocol progressively increased speed and intensity, which would enhance aerobic capacity, stroke volume, and muscular oxygen utilization[19,20]. Repeated practice also likely improved gait efficiency and muscle endurance, allowing children to walk farther before fatiguing. The use of mirrors and verbal cues may have additionally encouraged better posture and effort. In sum, treadmill training appears to recondition the cardiovascular-pulmonary system and lower‑limb musculature, translating into larger 6MWT distances[21].
In contrast treadmill training did not show any additional effect for constipation. Both groups showed significant within‑group reductions in Constipation Assessment Scale (CAS) scores over time, but there were no significant between‑group differences at any time point (p=0.16). There multiple factor contributing in the constipation among usually related to mobility, muscle tone, diet, etc. and the evidence suggests that targeted interventions are needed. The Awan et al. (2021) reported that a progressive physical therapy exercise program significantly increase defecation frequency and lower CAS scores in spastic CP[15]. Similarly, 6 weeks of daily stretching reduced both spasticity and constipation severity in CP children[21]. In the current study, both groups received stretching, core and gait exercises (Group B) or these plus treadmill (Group A). The lack of difference in improved constipation was likely due to the stretching and weight bearing exercises, which are known to improve abdominal and pelvic mobility[15,21]. Treadmill walking addition, even at moderate intensity may not sufficiently engage core musculature or alter autonomic tone to markedly affect gastrointestinal motility. Thus, the current study suggests that while treadmill training enhances cardiopulmonary fitness, additional or specialized interventions are still needed to address constipation in CP.
The current findings of endurance are similar as previous reports that gait training enhances functional capacity in CP. Although most literature has focused on speed or gait rather than 6MWT distance, but it suggest that repetitive treadmill exercise promotes cardiovascular conditioning and neuromuscular adaptations in CP[19], supporting current finding observation of improved endurance. The current results also suggest that even home-based walking programs improve 6-MWT distance in CP[21]. In short, the evidence consistently indicates that progressive treadmill training is an effective means to increase endurance in ambulatory children with CP.
In contrast, research on relationship between exercise and constipation among CP is limited. Since in current study treadmill group did not show any difference from the CPT in CAS outcomes, it suggests that the moderate intensity aerobic exercises did not add benefit for constipation, consistent with the evidence that aerobic exercise alone has limited direct impact on gut motility in CP. This highlights that stretching exercises and proper positioning reduce tone or abdominal massage directly stimulate the abdomen seem more effective for constipation than generic endurance training[15,21].
The exercise generally can stimulate intestinal motility via increased abdominal pressure and autonomic changes, but this effect may be minimum unless abdominal muscles are strongly engaged. The treadmill protocol focused on gait and kept sessions relatively brief and children held onto support bars, which might limit trunk muscle activation. In contrast, targeted stretching and core exercises more directly mobilize the abdomen and reduce hypertonicity, which can free up the bowel. Indeed, prior work shows a strong correlation between reduced spasticity and improved defecation[21]. Because conventional therapy likely addressed muscle tone and flexibility, both groups showed some improvement in CAS. However, treadmill training itself probably did not provide additional benefits beyond those effects. Therefore, findings suggest that treadmill training's primary physiological impact was on cardiopulmonary function rather than on neural or visceral factors governing bowel function.
These results have practical significance for CP management that progressive treadmill training can meaningfully enhance functional mobility and endurance in spastic diplegic children (GMFCS I-II). Improved walking endurance may translate into greater participation in play, school, and daily activities, and could reduce secondary health risks associated with inactivity[19,20]. On the other hand, because the treadmill did not measurably improve constipation, so a multimodal bowel program should be maintained including stretching, positioning, hydration, diet, perhaps abdominal massage alongside aerobic exercise. In practice, combining treadmill training with the conventional PT used here would produce comprehensive effects like better endurance from the treadmill plus reduced spasticity and improved gut motility from stretches and core exercises.
Limitations: The adherence and effort on the treadmill were monitored but not formally quantified, which could influence outcomes. To determine the combine effect of interventions on both variables, the sample size was limited.
CONCLUSIONThe treadmill training is an effective intervention for improving cardiorespiratory endurance in children with cerebral palsy, but it does not appear to independently effective for constipation outcomes. Therefore, a comprehensive rehabilitation approach combining treadmill training with conventional therapy and targeted bowel management strategies is recommended to optimize both functional mobility and gastrointestinal health in this population.
DECLARATIONS & STATEMENTSAuthor's Contribution
SS and RU: conception, design, and manuscript writing.
SS and OFM: supervision and critical revision.
SS: substantial contributions to the conception and design of the study.
SA and OFM: acquisition of data for the study.
SA, RU, OFM: interpretation of data for the study.
SS and SA: analysis of the data for the study.
SS and OFM: drafted the work.
SS, SA, RU, and OFM: revised it critically for important intellectual content.
SS, SA, RU, and OFM: final approval of the version to be published and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors contributed to the article and approved the submitted version.
Ethical Statement:
The study was conducted at Rahman Medical Institute (RMI)(RMI/30-11-2023) and Akbar Kare Institute (AKI) (AKI-PT/2023-12) Peshawar from Jan 2024 to May 2024.
AI Use Statement
The authors utilized ChatGPT for language editing and employed Python in conjunction with Gemini via Google Colab for figure generation. All content, analyses, and interpretations were thoroughly reviewed, verified, and approved by the authors.
Consent Statement
Written informed consent was obtained from all participants prior to data collection and for publication. The authors confirm that all participants voluntarily agreed to participate and that their confidentiality and privacy have been maintained throughout the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
None to declare.
Funding Sources
None to declare.
Conflicts of Interest
None to declare.
- Patel DR, Neelakantan M, Pandher K, Merrick J. Cerebral palsy in children: a clinical overview. Transl Pediatr. 2020;9(Suppl 1):S125-s35. [CrossRef] [PubMed]
- Marpole R, Blackmore AM, Gibson N, Cooper MS, Langdon K, Wilson AC. Evaluation and management of respiratory illness in children with cerebral palsy. Front Pediatr. 2020;8:333. [CrossRef] [PubMed]
- Ghafoor F, Fatima K, Fawad M, Munawar A, Baig MJ, Ahmad Z. Effectiveness of treadmill training alone versus treadmill training with external clues on improving gait and functional ability in parkinson's patient: improving gait and functional ability in parkinson's patient. Pak J Health Sci. 2023;4(10):105-10. [CrossRef]
- Rajesh S, Kanniappan V, Kanna BS, Veeragoudhaman T. Comparing the effects of virtual reality breathing exercise and incentive spirometry exercise on improving pulmonary function in children with spastic diplegic cerebral palsy. Cureus. 2024;16(4). [CrossRef] [PubMed]
- Atia DT, Hassan MH. Efficacy of under water exercise on pulmonary function in cerebral palsied children. [CrossRef]
- Santos KP, Silva VMMD, Reis IFD, Aquino MRC, Lana MRV, Teixeira CMMF. Physical conditioning in children and adolescents with cerebral palsy: Systematic review and meta-analysis. J Bodyw Mov Ther. 2023;35:158-163. [CrossRef] [PubMed]
- Mattern-Baxter K, Looper J, Zhou C, Bjornson K. Low-intensity vs high-intensity home-based treadmill training and walking attainment in young children with spastic diplegic cerebral palsy. Arch Phys Med Rehabil. 2020;101(2):204-212. [CrossRef] [PubMed]
- Bjornson KF, Moreau N, Bodkin AW. Short-burst interval treadmill training walking capacity and performance in cerebral palsy: a pilot study. Dev Neurorehabil. 2019;22(2):126-133. [CrossRef] [PubMed]
- Dodd KJ, Foley S. Partial body-weight-supported treadmill training can improve walking in children with cerebral palsy: a clinical controlled trial. Dev Med Child Neurol. 2007;49(2):101-5. [CrossRef] [PubMed]
- Ochandorena-Acha M, Terradas-Monllor M, Nunes Cabrera TF, Torrabias Rodas M, Grau S. Effectiveness of virtual reality on functional mobility during treadmill training in children with cerebral palsy: a single-blind, two-arm parallel group randomised clinical trial (VirtWalkCP Project). BMJ Open. 2022;12(11):e061988. [CrossRef] [PubMed]
- Doğan H, Mutluay F. Effect of treadmill backward walking training on motor capacity in cerebral palsy: a randomized controlled study. Ann Rehabil Med. 2023;47(2):89-97. [CrossRef] [PubMed]
- Sinha P, Chaudhary V. Effect of Backward Treadmill Training Versus Conventional Therapies to Improve Functional Mobility in Children with Spastic Diplegic Cerebral Palsy. Int J Converg Healthc. 2024;4(1):11-5. [CrossRef]
- Willoughby KL, Dodd KJ, Shields N, Foley S. Efficacy of partial body weight-supported treadmill training compared with overground walking practice for children with cerebral palsy: a randomized controlled trial. Arch Phys Med Rehabil. 2010;91(3):333-9. [CrossRef] [PubMed]
- Reuter M, Rosenberger F, Barz A, Venhorst A, Blanz L, Roecker K, Meyer T. Effects on cardiorespiratory fitness of moderate-intensity training vs. energy-matched training with increasing intensity. Front Sports Act Living. 2024;5:1298877. [CrossRef] [PubMed]
- Reuter M, Rosenberger F, Barz A, Venhorst A, Blanz L, Roecker K, Meyer T. Effects on cardiorespiratory fitness of moderate-intensity training vs. energy-matched training with increasing intensity. Front Sports Act Living. 2024;5:1298877. [CrossRef] [PubMed]
- Gacto-Sánchez M, Lozano-Meca JA, Lozano-Guadalajara JV, Montilla-Herrador J. Concurrent validity of the 2-and 6-minute walk test in knee osteoarthritis. Knee. 2023;43:34-41. [CrossRef] [PubMed]
- Wong WK, Qin J, Bressington D, Yeung WF, Liu N, Ho BYW, Liang S, Li Y. Cross-cultural adaptation and psychometric validation of the constipation assessment scale among chinese adult psychiatric patients. Int J Environ Res Public Health. 2023;20(3):2703. [CrossRef] [PubMed]
- Kim OY, Shin YK, Yoon YK, Ko EJ, Cho SR. The effect of treadmill exercise on gait efficiency during overground walking in adults with cerebral palsy. Ann Rehabil Med. 2015;39(1):25-31. [CrossRef] [PubMed]
- Tauro R, Ganesh S, Vincent JG. Effect of cardiovascular endurance training on the exercise capacity and endurance in children with cerebral palsy. Cureus. 2024;16(6):e61595. [CrossRef] [PubMed]
- Alotaibi A, Ibrahim A, Ahmed R, Abualait T. Effectiveness of partial body weight-supported treadmill training on various outcomes in different contexts among children and adolescents with cerebral palsy: a systematic review and meta-analysis. Children (Basel). 2023;11(1):9. [CrossRef] [PubMed]
- Romeo DM, Venezia I, De Biase M, Sini F, Velli C, Mercuri E, Brogna C. The Use of the 6MWT for Rehabilitation in Children with Cerebral Palsy: A Narrative Review. J Pers Med. 2022;13(1):28. [CrossRef] [PubMed]

Submitted
Accepted
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 Sulaiman Shah, Sheeraz Ali, RizwanUllah, Osama Faisal Mahboob

This work is licensed under a Creative Commons Attribution 4.0 International License.
Authors retain copyright and grant the journal right of first publication and allows others to share the work with an acknowledgment of the work’s authorship and initial publication in this journal. No use, distribution or reproduction is permitted which does not comply with these terms.