Effectiveness of segmental stabilization and general lumber stabilization exercises in chronic low back pain: A randomized controlled trial
DOI:
https://doi.org/10.52567/trehabj.v9i01.93Keywords:
disability, functional disability, physical therapy, low back pain, segmental stabilization exercises, lumbar stabilization exercisesAbstract
Background: Chronic low back pain (CLBP) is a prevalent musculoskeletal condition that significantly impacts functional ability and quality of life. Exercise-based interventions are essential in managing CLBP by improving spinal stability and reducing pain. Segmental stabilization exercises (SSE) target deep stabilizing muscles, aiming to enhance motor control and reduce spinal micro-instability, whereas general lumbar stabilization (GLS) exercises focus on overall core muscle activation to improve spinal support.
Objective: to determine the effectiveness of segmental stabilization exercises and general stabilization exercises in chronic low back pain patients.
Methodology: A randomized controlled trial was conducted on n=44 participants with chronic low back pain patients at Isra University, Islamabad, and Benazir Bhutto Hospital, Rawalpindi, from January 2020 – August 2020. The participants were recruited through a non-probability convenient sampling technique and divided into two groups, n=22 participants in each group. The experimental group received Segmental Stabilization Exercises (SSE) while the control group received General Lumbar Stabilization (GLS). Visual Analogue Scale (VAS) was used to determine the severity or level of pain, a goniometer was used to measure the Range of Motion (ROM), Oswestry Disability Scale (ODI), was used to determine the severity or level of disability. The Friedman test with Wilcoxon was used within the group analysis whereas the Mann-Whitney U test was used for between the groups analysis.
Results: Both interventions SSE and GLS, significantly reduced (p<0.05) pain intensity and physical disability on ODI and its domains over time by the end of 4th week. Meanwhile, the between-group analysis revealed no statistically significant differences (p≥0.05).
Conclusion: SSE and GLSE significantly improve pain and disability scores over four weeks. However, the lack of significant between-group differences suggests that both interventions have comparable efficacy.
INTRODUCTION
Chronic low back pain (CLBP) is usually defined as pain in the back that persists for 7 to 12 weeks [1, 2]. It escalates linearly after 30 years of age until the 6th decade of life [3] and is more common in females compared to males [4]. CLBP is a restrictive condition may lead to a massive global burden that due to long absences from work and substantial workers' reimbursement and social security expenses due to work absences and retirement [5,6].
Though there are a lot of reasons leading to low back pain in many chronic cases, the cause is not known [7]. Postural issues, decrease in physical exercise, genetic issues, low levels of education along nutritional deficiencies are noteworthy risk factors of LBP [2]. Bodily workload escalates the risk of back ache [4]. Also, weakness of superficial abdominal and trunk muscles, and lack of control of deep trunk muscles, such as transversus abdominis (TrA) and lumbar multifidus (LM) is an important risk factor and strengthening of these muscles significantly improved CLBP and disability. CLBP patients usually reported delayed contractions of TrA [8].
Multi-disciplinary approach including pharmacological, surgical, and physical therapy is used to treat CLBP [9]. Exercise is a widely prescribed treatment, and it leads to improvement in function and work [10]. An intensive exercise program leads to the enhancement of bodily functions and has modest effects in the case of CLBP [9]. Furthermore, segmental stabilization exercises (SSE), [8] and general lumbar stabilization exercises (GLS) [11] are used to treat CLBP. Stabilization exercises improve neuromuscular control, strength, and endurance of muscles [11] while SSE also improves the timely activation of TrA and LM muscles [8]. These factors are central to the maintenance of dynamic trunk and spinal stability. Stabilization exercises are usually recommended for their safety and cost-effectiveness [11].
Although previous studies have investigated the effects of SSE and GLS in managing CLBP, limited research has examined their comparative effectiveness in a combined clinical and home-based setting with a follow-up beyond the supervised intervention phase. Most existing studies assess short-term outcomes within clinical settings, failing to determine whether improvements are sustained once patients transition to self-managed care. This study aims to address these gaps by comparing the effectiveness of SSE and GLS in CLBP rehabilitation, incorporating both supervised and home-based exercise phases, and assessing outcomes over four weeks.
METHODOLOGY
Design & Setting: A randomized control trial was conducted at the physical therapy department of Isra Institute of Rehabilitation Sciences (IIRS), Isra University Islamabad Campus. was after the approval of the Advanced Studies and Research Committee (IIRS/ASRC/OPT-008) of Isra University, Islamabad. The study was conducted from March 2019 – June 2022.
Selection criteria: The inclusion criteria for the recruitment in the study were males and females, between 15 to 60 years of age, and had chronic low back pain. While patient excluded with a history of back surgery, pregnancy, sciatica, any nerve root entrapment, vertebral bone fracture, stroke, spinal cord injury, intellectual disability, and rheumatologic disorders.
Sample Size: This sample size was n=44, calculated using a moderate effect size (f=0.35), with 80% power at a 5% significance level. A total of 60 subjects were evaluated for the study, out of which n=16 subjects were excluded for not meeting the inclusion criteria and unwillingness to participate in the study. The remaining n=44 participants were recruited through a non-probability convenient sampling technique and randomly divided into Segmental Stabilization Exercises (SSE) group (n=22), and Generalized Lumber Stabilization exercises (GLS) group (n=22) as shown in Figure 1.
Randomization & Blinding: The computerized randomization method by an independent researcher not involved in the assessment and management of the participant was used in this study. The allocation to the SSE group and the GLS group was through opaque sealed envelopes, which were opened only after participant enrolment. The blinding was not done as the individuals actively engaged in their assigned exercise interventions. To reduce performance bias, exercise logs of the home base plan were recorded in writing. Additionally, therapist blinding was not feasible since different exercise protocols were administered and remained a limitation, so follow the structured intervention protocols.
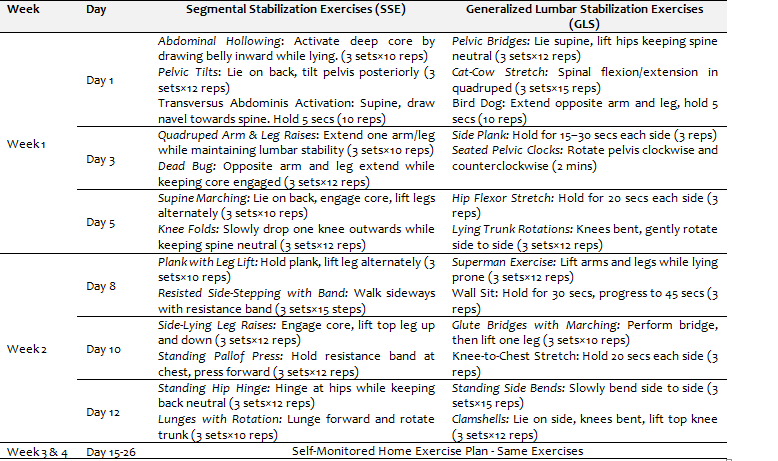
Intervention: The participants of the Segmental Stabilization exercise (SSE) performed a protocol, while the participants of the Generalized Lumbar Stabilization Exercises (GLS) group performed open and closed chain exercises. A detailed protocol is shown in Table 1. Each participant received a total of 3 sessions in a week, and the home care plan was guided by the treating physiotherapist. Each session lasted for 45 minutes and started in prone lying received 10 minutes of hot pack and TENS for two weeks. After two weeks, a Self-Monitored Home Exercise Plan of the Same Exercises was performed till 4th week. (table 1)
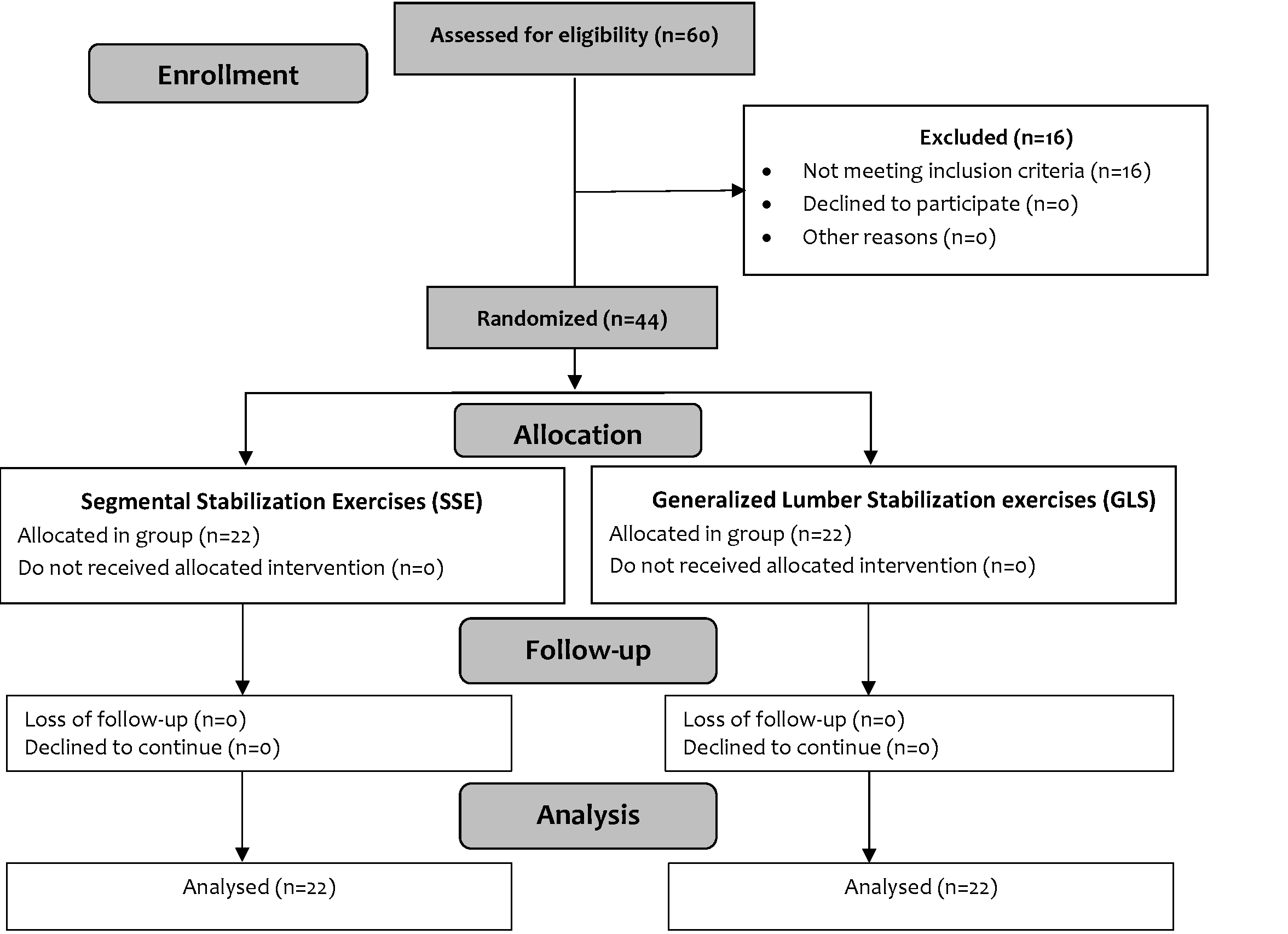
Figure 1: Consort diagram
Table 1: Intervention protocol segmental stabilization and generalized lumbar stabilization exercise plan
Data collection procedure: The general demographics data such as age, gender, BMI, level of physical activity, and occupation were collected at baseline. Physical activity was measured through the International Physical Activity Questionnaire Short Form -7 (IPAQ SF-7), which is a valid and reliable tool [13]. Visual Analogue Scale (VAS) was used to determine the severity or level of pain. The VAS is a valid and reliable tool [12] and consists of ten characteristics which include 0= no pain and 10= severe pain. The Range of Motion (ROM) of lumbar flexion, extension, lateral right-side flexion, and lateral left-side flexion. The ROM was measured through a goniometer, which is a valid and reliable tool [14]. Oswestry Disability Scale (ODI) was used to determine the severity or level of disability and is a valid and reliable tool [15]. In ODI, 0 indicates no disability whereas 50 indicates severe disability.
Statistical Analysis: The descriptive statistics, mean, standard deviation, frequency, and percentages. As the VAS and total score of ODI were not normally distributed on The Shapiro–Wilk test and ODI's domains were in ordinal scale. The non-parametric test was used for data analysis. Therefore, the Mann-Whitney U test was used between the group analyses whereas the Friedman test with the Wilcoxon test were used within the group analysis. To determine the effectiveness of treatment protocols, the level of significance was set at p<0.05, and SPSS 21 was used to analyze the data.
RESULTS
The mean age of participants was 44.04 ±10.52 years. The mean height was 1.615±0.06 m, while the mean weight was 70.52±12.02 kg. The combined mean BMI was 26.89±4.29kg/m2. These values represent the overall characteristics of the study participants across both experimental (SSE) and control (GLS) groups.
Table 2: Within group changes Pain (VAS) and Disability (ODI)

Within-group analysis, using the Friedman test with Wilcoxon signed rank test for pairwise comparison, showed that both interventions Segmental Stabilization Exercises (SSE) and Generalized Lumbar Stabilization Exercises (GLS), significantly reduced (p<0.05) pain intensity as well as physical disability on ODI and its domains over time by the end of 4th week.
Between-group analysis using the Mann-Whitney U test revealed no statistically significant differences (p≥0.05) in VAS and ODI domains between SSE and GLSE at any time point (table 3).
Table 3: Between group differences (Mann Whitney U Test)

DISCUSSION
The purpose of the study was to determine the effectiveness of segmental stabilization exercises and general lumbar stabilization exercises on pain and disability in patients with chronic low back pain with lower back pain over four weeks. It was hypothesized that SSE would be more effective as compared to GLS, however, based on the results hypothesis was rejected. The efficacy of stabilization exercises in improving core stability, decreasing pain, and improving functional outcomes.
The significant reduction in pain intensity, as measured by VAS, is supported by prior studies suggesting that lumbar stabilization exercises improve neuromuscular control, thereby decreasing pain perception [16, 17]. Furthermore, the observed decrease in Oswestry Disability Index (ODI) scores is consistent with findings from Mahmood et al. (2022), who reported substantial improvements in physical function following core stabilization training [18].
The results of the study showed significant improvement in pain, and disability after segmental stabilization exercises measured through VAS, and ODI which is supported by the previous studies, in which SSE significantly improved pain, and ROM and reduced functional disability [19, 20, 21]. The possible reason for the improvement is exercising TrA and LM, which improves muscle activation, and segmental protective function and reduces stress on the lumbar [8]. Thus, proper segmental stabilization exercises are effective in improving pain, ROM, and thus disability.
According to the result of the recent study pain, ROM, and disability were significantly improved after general stabilization exercise. The results of this study are in coherence with the previous literature, which reported significant improvement in pain, ROM, and disability after stabilization exercises [11]. The improvement that occurred may be due to the open-chain and closed-chain exercises, which strengthen the TrA and LM muscles. Therefore, stabilization exercises reduced pain and ROM and thus disability because of strengthening and activation of TrA and LM muscles [22]. In low back pain, the delayed contractions of the TrA muscle make the trunk unstable and lead to reduced postural and motor control and the working of spinal muscles. Also, closed-chain exercises, which are performed on unstable surfaces are more effective in improving postural balance [23].
Furthermore, no significant difference was observed between SSE and GLS in improving pain, ROM, and disability. The previous study supported the findings of the current study, which reported segmental stabilization exercises are equally effective to other physiotherapy treatments such as lumbar stabilization exercises [24]. The possible reason for the non-significant difference could be due to the techniques used. Both treatment procedure focuses on the activation of TvA and LM muscles [8, 23]. Also, stabilization exercises strengthen the superficial and deep muscles of the trunk and abdomen which provides stability and reduces the pain and thus disability [11]. The non-significant between-group differences may also suggest that SSE and GLSE may have similar therapeutic effects [25, 26].
The sample size of the current study was smaller due to time constraints, so this study lacks generalizability to a wider population.
CONCLUSION
Both SSE and GLSE significantly improve pain and disability scores over four weeks. However, the lack of significant between-group differences suggests that both interventions have comparable efficacy. The inclusion of a home-based follow-up phase stresses the practicality of self-managed care after supervised intervention, providing insights into the sustainability of improvements beyond clinical settings. Future studies should explore long-term effects and adherence strategies to optimize patient outcomes in self-managed rehabilitation programs.
DECLARATIONS & STATEMENTS
Author’s Contribution
SMZ: substantial contributions to the conception and design of the study.
SMZ: acquisition of data for the study.
SMZ and FMZ: analysis of the data for the study.
AA, SMZ and MA: interpretation of data for the study.
AA, SMZ, MA, HA, and FMZ: drafted the work.
AA, SMZ, MA, HA, and FMZ: revised it critically for important intellectual content.
AA, SMZ, MA, HA, and FMZ: final approval of the version to be published and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors contributed to the article and approved the submitted version.
Ethical Statement
The study was conducted after the approval of the Advanced Studies and Research Committee IIRS/ASRC/OPT-008 of Isra University, Islamabad.
Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
None to declare.
Funding Sources
None to declare.
Conflicts of Interest
None to declare.
REFERENCES
- Andersson GB. Epidemiological features of chronic low-back pain. The lancet. 1999;354(9178):581-5. [CrossRef] [PubMed]
- Lionel A. Risk factors forchronic low back pain. Community Med Health Educ. 2014;4(271):2161-0711. [CrossRef]
- Meucci RD, Fassa AG, Faria NMX. Prevalence of chronic low back pain: systematic review. Revista de saude publica. 2015;49:73. [CrossRef] [PubMed]
- Shiri R, Falah‐Hassani K, Heliövaara M, Solovieva S, Amiri S, Lallukka T, et al. Risk factors for low back pain: a Population‐Based longitudinal study. Arthritis Care Res (Hoboken) .. 2019;71(2):290-9. [CrossRef] [PubMed]
- Meucci D, Fassa AG, Paniz V, Silva MC, Wegman DH. Increase of chronic low back pain prevalence in a medium-sized city of southern Brazil. BMC musculoskeletal disorders. 2013;14(1):1-11. [CrossRef] [PubMed]
- Yiengprugsawan V, Hoy D, Buchbinder R, Bain C, Seubsman S-a, Sleigh AC. Low back pain and limitations of daily living in Asia: longitudinal findings in the Thai cohort study. BMC musculoskeletal disorders. 2017;18(1):1-7. [CrossRef] [PubMed]
- Chiodo AE, Bhat SN, Van Harrison R, Shumer GD, Wasserman RA, Park P, Patel RD, Van Harrison R, Proudlock AL, Rew KT. Low back pain [Internet]. Ann Arbor (MI): Michigan Medicine University of Michigan; 2020 Nov. [PubMed]
- Soundararajan LR, Thankappan SM. Efficacy of the multifidus retraining program in computer professionals with chronic low back pain. Asian Spine J. 2016 Jun;10(3):450-6. [CrossRef] [PubMed]
- França FR, Burke TN, Hanada ES, Marques AP. Segmental stabilization and muscular strengthening in chronic low back pain: a comparative study. Clinics. 2010;65(10):1013-7. [CrossRef] [PubMed]
- Bogduk N. Management of chronic low back pain. Med J Aust . 2004;180(2):79-83. [CrossRef] [PubMed]
- Rainville J, Hartigan C, Martinez E, Limke J, Jouve C, Finno M. Exercise as a treatment for chronic low back pain. Spine J . 2004;4(1):106-15. [CrossRef] [PubMed]
- Suh JH, Kim H, Jung GP, Ko JY, Ryu JS. The effect of lumbar stabilization and walking exercises on chronic low back pain: a randomized controlled trial. Medicine (Baltimore). 2019;98(26). [CrossRef] [PubMed]
- Craig C, Marshall A, Sjostrom M, Bauman A, Lee P, Macfarlane D, et al. International physical activity questionnaire-short form. J Am Coll Health. 2017;65(7):492-501.
- IOde Boer AG, van Lanschot JJ, Stalmeier PF, van Sandick JW, Hulscher JB, de Haes JC, et al. Is a single-item visual analogue scale as valid, reliable and responsive as multi-item scales in measuring quality of life? Qual Life Res. 2004;13(2):311-20. [CrossRef] [PubMed]
- Carey MA, Laird DE, Murray KA, Stevenson JR. Reliability, validity, and clinical usability of a digital goniometer. Work. 2010;36(1):55-66. [CrossRef] [PubMed]
- Vianin M. Psychometric properties and clinical usefulness of the oswestry disability index. J Chiropr Med . 2008;7(4):161-3. [CrossRef] [PubMed]
- Taulaniemi A, Kankaanpää M, Tokola K, Parkkari J, Suni JH. Neuromuscular exercise reduces low back pain intensity and improves physical functioning in nursing duties among female healthcare workers, secondary analysis of a randomised controlled trial. BMC Musculoskelet Disord. 2019;20(1):328. [CrossRef] [PubMed]
- Porwal S, Rizvi MR, Sharma A, Ahmad F, Alshahrani MS, Raizah A, et al. Enhancing functional ability in chronic nonspecific lower back pain: the impact of emg-guided trunk stabilization exercises. Healthcare (Basel). 2023;11(15). [CrossRef] [PubMed]
- Mahmood W, Ahmed Burq HSI, Ehsan S, Sagheer B, Mahmood T. Effect of core stabilization exercises in addition to conventional therapy in improving trunk mobility, function, ambulation and quality of life in stroke patients: a randomized controlled trial. BMC Sports Sci Med Rehabil. 2022;14(1):62. [CrossRef] [PubMed]
- O'Sullivan PB, Phyty GDM, Twomey LT, Allison GT. Evaluation of specific stabilizing exercise in the treatment of chronic low back pain with radiologic diagnosis of spondylolysis or spondylolisthesis. Spine (Phila Pa 1976).1997;22(24):2959-67. [CrossRef] [PubMed]
- Hides JA, Jull GA, Richardson CA. Long-term effects of specific stabilizing exercises for first-episode low back pain. (Phila Pa 1976).2001; 26(11):e243-e8. [CrossRef] [PubMed]
- Bhadauria EA, Gurudut P. Comparative effectiveness of lumbar stabilization, dynamic strengthening, and Pilates on chronic low back pain: randomized clinical trial. J Exerc Rehabil . 2017; 13(4):477. [CrossRef] [PubMed]
- Özüdoğru A, Gelecek N. Effects of closed and open kinetic chain exercises on pain, muscle strength, function, and quality of life in patients with knee osteoarthritis. Rev Assoc Med Bras (1992). 2023;69(7):e20230164. [CrossRef] [PubMed]
- Yun K, Lee S, Park J. Effects of closed chain exercises for the lumbar region performed with local vibration applied to an unstable support surface on the thickness and length of the transverse abdominis. J Phys Ther Sci . 2015; 27(1):101-3. [CrossRef] [PubMed]
- Rackwitz B, de Bie R, Limm H, von Garnier K, Ewert T, Stucki G. Segmental stabilizing exercises and low back pain. What is the evidence? A systematic review of randomized controlled trials. Clin Rehabil .2006;20(7):553-67. [CrossRef] [PubMed]
- Suh JH, Kim H, Jung GP, Ko JY, Ryu JS. The effect of lumbar stabilization and walking exercises on chronic low back pain: A randomized controlled trial. Medicine (Baltimore). 2019;98(26):e16173. [CrossRef] [PubMed]
- Boucher J-A, Preuss R, Henry SM, Dumas J-P, Larivière C. The effects of an 8-week stabilization exercise program on lumbar movement sense in patients with low back pain. BMC Musculoskeletal Disorders. 2016;17(1):23. [CrossRef] [PubMed]

Submitted
Accepted
Published
How to Cite
Issue
Section
License
Copyright (c) 2025 Amnah Anum, Summaiya Malik Zaman, Muhammad Ahmad

This work is licensed under a Creative Commons Attribution 4.0 International License.
Authors retain copyright and grant the journal right of first publication and allows others to share the work with an acknowledgment of the work’s authorship and initial publication in this journal. No use, distribution or reproduction is permitted which does not comply with these terms.