Barriers to utilizing low vision devices among non-users with low vision: A cross-sectional study
DOI:
https://doi.org/10.52567/trehabj.v7i04.38Keywords:
blindness, low-vision, low vision devicesAbstract
Background: By recognizing and comprehending the obstacles that prevent low vision devices (LVDs) from being used effectively, the burden of blindness can be reduced.
Objective: To find the barriers to the utilization of low-vision devices (LVDs) among non-users in patients with low vision.
Methods: A cross-sectional study was conducted in the low vision department of Al-Shifa Trust Eye hospitals in Rawalpindi, Pakistan for a duration of six months from July 2021 to December 2021. Low-vision individuals with visual acuity ˂6/18 fulfilling the criteria of low vision and prescribed low-vision devices over the period of 6 months but not using them were included in this study. A total of n=420 patients were evaluated for eligibility, out of which n=255 were prescribed low-vision devices due to low vision. The data was collected on the self-structured questionnaire in accordance with the tenets of Helsinki’s declaration.
Results: Out of n=255, a total of n=105 were using (acceptance) and n=150 were not using (non-acceptance) the LVDs. Out of 15 possible barriers, fear of being perceived as blind N=120(80%) is the major cause of non-acceptance of devices among low-vision individuals. It was followed by difficulty in handling low-vision devices n=106(70.7%) and low affordability n=106(70.7%). While fear of loss of job 2(1.3%) was selected as the least occurring problem in non-acceptance of devices.
Conclusions: Leading barriers included stigma, lack of information, concern over losing one's job, fear of being viewed as blind, and low necessity.
INTRODUCTION
World Health Organization (WHO), defines low vision patient as a person having visual acuity of less than 20/60 to light perception or having a visual field of less than 10° from the point of fixation, even after receiving medical, surgical, and/or standard refractive correction but he/she is capable of performing the activities of daily life [1, 2]. According to the Vision Loss Expert Group (VLEG), 253 million individuals worldwide are visually impaired. People with vision impairment make up about eighty-nine percent of the population in low- and middle-income nations (LMIC) [3, 4].
There is a connection between visual impairment (VI) and falling, fractures, and a higher mortality rate. Psychological issues, such as depression and anxiety, are more likely to develop in those with visual impairment. People with reduced vision can improve their quality of life by receiving vision rehabilitation, which instructs them on how to use their remaining eyesight more effectively [5]. They might regain or maintain their independence with the aid of various visual and adaptive aids. Devices for people with limited vision are an efficient way to provide visual rehabilitation, according to the literature [6]. Despite the fact that low vision services help patients by enhancing their quality of life [7], awareness of the services among eye care professionals (ECPs) and low vision service uptake remain low, even in developed nations [8].
The need for low vision services and their uptake are not aligned. A number of barriers may make it more difficult for people to access low vision services including limited low vision services or there may not be enough experts with the necessary training to offer these services [9]. Some studies reported that social stigma, difficulty in handling the devices, lack of knowledge, fear of loss of job, poor communication between eye care professionals and patients, low affordability and fear of being viewed as blind also appear as a main barrier [10-12].
Many low vision patients have been prescribed low vision devices, but they are not using them due to some barriers. By being aware of these obstacles, campaigns can be developed to raise awareness among patients, healthcare workers, and public. It will also motivate patients to use their devices in their daily life activities so that their quality of life may improve, and they can live an independent life. So, this study aims to assess the barriers faced by low-vision patients in utilizing low-vision aids.
METHODOLOGY
This cross-sectional study was conducted from July 2021 to December 2021 at the low vision department of Al-Shifa Trust Eye Hospital, Rawalpindi Pakistan (ASTEH) after approval from Ethical Review committee (ERC-72/AST-21). This study included patients who were prescribed low-vision devices (LVD) and had visual acuity of less than 6/18. The patients of age fewer than 10 years, having distance acuity of less than 1/60, and low intellectual levels were excluded from this study.
The data was collected through non-probability sampling technique. A total of n=420 participant was evaluated for the selection criteria, n=255 patients were prescribed with low vision aids (LVA). Out of which n=150 patients (not using LVA) fulfilled the inclusion criteria and remaining n=105 (using LVA) were excluded from the study.
The outcome variable of this study was barriers to using low vision aids (LVAs), which was measured by asking those questions that were scaled into yes and no. The first section of the questionnaire gathered data on the patients' socio demographics while inquiries on their eye health and low vision aids were part of the second section. The last part consists of questions about the barriers to low-vision devices, which was based on similar studies published previously (5).
Before participation in this study, verbal informed consent was also taken from every individual. At every stage of the study, the confidentiality of the patient's data was upheld, and the ethical standards of research were properly considered. All the data was collected under the supervision of experts in this field. Distance and near visual acuity of the patient was recorded using an Early Treatment Diabetic Retinopathy Study (ETDRS) chart and Lighthouse near vision chart respectively. After that, visual acuity with the prescribed low vision devices was recorded with which vision gets improved and then the questionnaires was filled for not using it to find the barriers. For the patients of age, less than 16 years’ parents or caregivers were the main decision-makers who answer the questions on the behalf of the children.
The Statistical Package for Social Sciences (SPSS) version 21 was used to enter and analyze the responses. The tables and charts were used to depict the frequency and percentages for categorical variables and the mean standard deviation for continuous data.
RESULTS
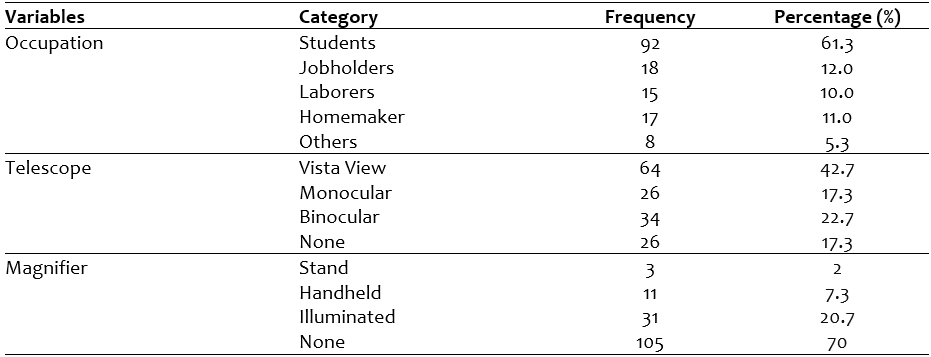
A total of n=72(48.0%) was male and remaining n=78(52%) was female. The n=83(55.3%) of participant’s age were between 17-25 years, while n=39(26%) was between 26-45 years and remaining n=28(18.7%) had age more than 45 years. The other demographic characteristics of study participants can be seen in table 1.
Table 1: Demographic characteristics of the patients
The major causes of low vision reported were maculopathy n=39 (26%), RP n=22(14.7%), Albinism n=16(10.7%), Diabetic retinopathy n=10(6.7%), Retinal detachment n=10(6.7%) and Nystagmus n=10 (6.7%), cataract n=9 (6%) Glaucoma n=9 (6%), ARMD n=7(4.7%) and others n=18 (11.8%).
The mean score of best-corrected distance visual acuity (BCDVA) of the left and right eyes were 1.07±0.36 and 1.04±0.32 diopters respectively. The mean near vision was1.48±0.84diopters.
Fear of being perceived as blind N=120 (80%) followed by difficulty in handling the device N=106 (70.7%) and low affordability N=106 (70.7%), visual fields restriction N=103 (68.7%), discomfort N= 94 (62.7%) were the major barriers for not using low vision devices. The other barriers can be seen in table 2. Most patients were prescribed by Telescopes followed by filters and non-optical devices. (Figure 1)
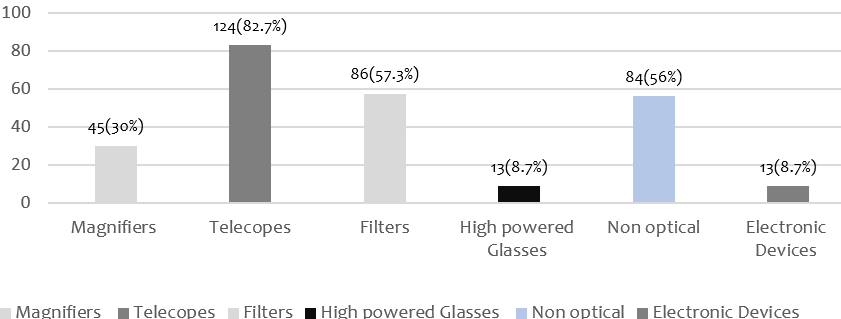
Figure 1: Low-Vision Devices
Table 2: Frequency distribution of Barriers perceived using Low vision devices

DISCUSSION
Assessing the barriers patients with low vision have utilizing low-vision devices was the main goal of this study. It was seen that many of the patients are afraid of being perceived as blind by using low-vision devices which include telescopes, filters, non-optical aids and magnifiers. This is followed by difficulty in handling low-vision devices, and some cannot afford these devices due to other reasons.
Sylvester et al [13] found that most barriers in low vision patients include lack of awareness, high cost of low vision devices, and social stigma or denial related to low vision. However, this study [13] was an organizational study i.e, the response of health care practitioners was recorded instead of low vision patients, and data was collected from the practitioners from different organizations. Even with this research model the major barrier in the study remains the denial and unacceptability in social platforms along with the high cost of low-vision devices.
K S Khimani et al [14] stated that social anxiety and depression (76%) and denial of the need for low vision aids (71%) are the major cause of barriers to the utilization of the devices. Similarly, Charles Walter et al [15] also reported that the psychological and economic barriers remain at large in low-vision patients who are seeking and availing low-vision related management. Interestingly, in another report, the rate of non-acceptance was high in the patients that have retinitis pigmentosa and high refractive error as the use of low vision devices reduces the already restricted visual fields and impairs depth[10]. The restricted visual field in the current study was found to be the 4th major barrier in the non-acceptance of low vision aids.
Previous studies at different times and regions also showed that the major cause of low vision is macular pathologies, then comes retinitis pigmentosa and diabetic retinopathy [10,16]. Wong et al [17] also added that in East Asia, refractive error is likewise the main factor contributing to visual loss. Age-related macular degeneration is the main contributing factor, according to J. Lindsey et al. [18] The majority of mentioned studies agree with the current study on the leading cause of low vision in different areas and regions.
Because of decreased visual acuity, the patients could not self-administer the questionnaire. The questions were thus read loudly, and responses were recorded according to observation of researcher. This technique may have introduced a bias that has affected the patient’s responses. This study was cross-sectional, further longitudinal studies are required to determine the leading barriers in utilizing low vision devices. The sample size of the current study was low and the data for the barrier identification was not obtained from the users of LVAs.
CONCLUSION
The current study revealed that leading barriers included stigma, lack of information, concern over losing one's job, fear of being viewed as blind, and low necessity. The burden of blindness can be lessened by addressing the underlying factors that lead to the underuse of low vision devices.
DECLARATIONS & STATEMENTS
Author’s Contribution
IT: substantial contributions to the conception and design of the study.
IT and FA: acquisition of data for the study.
MT and AS: interpretation of data for the study.
SI: analysis of the data for the study.
SI and AS: drafted the work.
IT, FA, MT, SI and AS: revised it critically for important intellectual content.
IT, FA, SI, MT and AS: final approval of the version to be published and agreement to be accountable for all aspects.
of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors contributed to the article and approved the submitted version.
Ethical Statement
The study was conducted after getting approval from the Research Ethical committee of Al-Shifa Trust Eye Hospital, Rawalpindi (ERC-72/AST-21).
Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
None to declare.
Conflicts of Interest
None to declare.
Funding
None to declare.
REFERENCES
1. Bittner AK, Wykstra SL, Yoshinaga PD, Li T. Telerehabilitation for people with low vision. Cochrane Database Syst Rev. 2015.31;8:CD011019 [CrossRef] [PubMed]
2. Wang S, Liu Y, Du Y, Bao H, Zhu J, Liu X. Influencing factors of low vision 2 years after vitrectomy for proliferative diabetic retinopathy: an observational study. BMC Ophthalmol. 2023;23(1):1-7. [CrossRef] [PubMed]
3. Chiang PP-C, O’Connor PM, Le Mesurier RT, Keeffe JE. A global survey of low vision service provision. Ophthalmic Epidemiol 2011;18(3):109-21. [CrossRef] [PubMed]
4. Javed M, Afghani T, Zafar K. Barriers to low vision services and challenges faced by the providers in Pakistan. J. Korean Clin. Health Sci.2015;3(3):399-408.
5. Bourne RR, Flaxman SR, Braithwaite T, Cicinelli MV, Das A, Jonas JB, et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: a systematic review and meta-analysis. Lancet Glob. Health 2017;5(9):e888-e97.[CrossRef] [PubMed]
6. Manjari K, Singhal K, Verma M, Singal G. AnimNet: An Animal Classification Network using Deep Learning. Machine Learning Algorithms and Applications. 2021:247-65. [CrossRef]
8. Khan SA, Shamanna B, Nuthethi R. Perceived barriers to the provision of low vision services among ophthalmologists in India. Indian J Ophthalmol 2005;53(1):69-75. [CrossRef] [PubMed]
9. Matti AI, Pesudovs K, Daly A, Brown M, Chen CS. Access to low‐vision rehabilitation services: barriers and enablers. Clin Exp Optom 2011;94(2):181-6. [CrossRef] [PubMed]
10. Sivakumar P, Vedachalam R, Kannusamy V, Odayappan A, Venkatesh R, Dhoble P, et al. Barriers in utilisation of low vision assistive products. Eye. 2020;34(2):344-51. [CrossRef] [PubMed]
11. Overbury O, Wittich W. Barriers to low vision rehabilitation: the Montreal Barriers Study. Investig. Ophthalmol. Vis. Sci. 2011;52(12):8933-8. [CrossRef] [PubMed]
12. Köberlein J, Beifus K, Schaffert C, Finger RP. The economic burden of visual impairment and blindness: a systematic review. BMJ open. 2013;3(11):e003471. [CrossRef] [PubMed]
13. Kyeremeh S, Mashige KP. Availability of low vision services and barriers to their provision and uptake in Ghana: practitioners’ perspectives. Afr Health Sci 2021;21(2):896-903. [CrossRef] [PubMed]
14. Khimani KS, Battle CR, Malaya L, Zaidi A, Schmitz-Brown M, Tzeng H-M, et al. Barriers to low-vision rehabilitation services for visually impaired patients in a multidisciplinary ophthalmology outpatient practice. J. Ophthalmol. 2021;2021. [CrossRef] [PubMed]
15. MJ Leys, R Althouse, C Walker, H Humble, JV Odom; West Virginia Survey of Visual Health: Low Vision and Barriers to Access . Invest. Ophthalmol. Vis. Sci. 2004;45(13):1122.
16. Keeffe JE, Lovie‐Kitchin JE, Taylor HR. Referral to low vision services by ophthalmologists. Aust. N.Z. j. ophthalmol. 1996;24(3):207-14. [CrossRef] [PubMed]
17. Wong TY, Zheng Y, Jonas JB, Flaxman SR, Keeffe J, Leasher J, et al. Prevalence and causes of vision loss in East Asia: 1990–2010. Br J Ophthalmol 2014;98(5):599-604.[CrossRef] [PubMed]
18. Lindsay J, Bickerstaff D, McGlade A, Toner A, Jackson A. Low vision service delivery: an audit of newly developed outreach clinics in Northern Ireland. Ophthalmic Physiol Opt 2004;24(4):360-8. [CrossRef] [PubMed]
Submitted
Published
Issue
Section
License
Copyright (c) 2023 Iqra Tariq, Fareeha Ayyub, Mehreen Tanveer, Shahid Iqbal, Arooshia Shahzadi

This work is licensed under a Creative Commons Attribution 4.0 International License.
Authors retain copyright and grant the journal right of first publication and allows others to share the work with an acknowledgment of the work’s authorship and initial publication in this journal. No use, distribution or reproduction is permitted which does not comply with these terms.